4 Supportive Health Care
Learning Objectives
By the end of this chapter, you should be able to:
- Identify symptoms of infectious diseases that are common during early childhood.
- Outline criteria for exclusion from care for ill children and staff.
- Describe considerations programs must make regarding caring for children that are mildly ill.
- Recall licensing requirements for handling medication in early care and education programs.
- Explain the communication about illness that should happen between families and early care and education programs.
 |
Licensing Regulations WAC regulations that relate to this chapter include:
110-300-0205 – CHILD, STAFF, AND HOUSEHOLD MEMBER ILLNESS[1]
246-110 – ILLNESS REPORTING REQUIREMENTS[2] WAC 246-110-001 The rules in this chapter identify certain contagious diseases that may affect children, or others who are susceptible, in schools, and childcare centers. When an outbreak or potential outbreak of a contagious disease is identified in a school or childcare center, the rules in this chapter identify what schools, childcare centers and local health officers may do to control or prevent a potential outbreak of the contagious disease. These rules are in addition to other requirements imposed by chapter 246-100 WAC, Communicable and certain other diseases and chapter 246-101 WAC, Notifiable conditions. These rules do not require school or childcare center personnel to diagnose or treat children.
WAC 246-110-010
The definitions in this section apply throughout this chapter unless the context clearly requires otherwise:
WAC 246-100-020
110-300-0215 – MEDICATION
|
Illness in Early Care and Education Programs
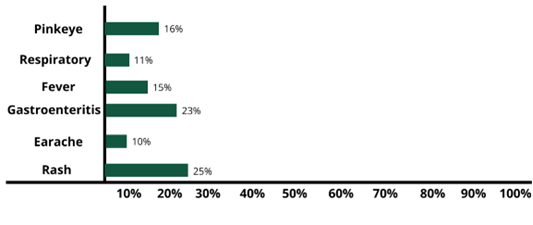
The most frequent infectious disease symptoms that are reported by early care and education settings are sore throat, runny nose, shortness of breath or cough, fever, vomiting and diarrhea (gastroenteritis), earaches, and rashes.
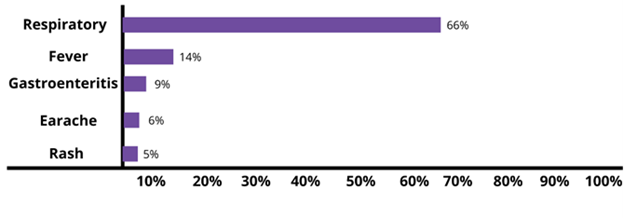
However, these are not the symptoms that necessarily lead to children staying home. In fact, although respiratory symptoms are most common, it’s rashes and gastrointestinal disease that more often keep children from attending their early education programs. This is more a reflection of exclusion policies than real risk of serious illness.[3]
It’s important for early childhood programs to identify illness accurately and respond in ways that protect all children and staff health (whether it be to allow them to stay in care or to exclude them from care).
Infectious Illness
Most children with mild illnesses can safely attend an early learning program “Many health policies concerning the care of ill children [including exclusion policies] have been based upon common misunderstandings about contagion, risks to ill children, and risks to other children and staff. Current research clearly shows that certain ill children do not pose a health threat. Also, the research shows that keeping certain other mildly ill children at home or isolated at the child care setting will not prevent other children from becoming ill.”[4]
It is extremely important for early childhood educators to know what symptoms to look for and when to separate and/or have a child stay home with an illness. In the Resources section, you will find Infectious Disease Information that describes the symptoms and effects of illnesses that children and adults experience.
Exclusion Policies
When you are familiar with different infectious diseases, it’s easier to identify them in children and adults and determine if those affected should be excluded from the early care and education program. The Resources for Washington State Infections Disease contains information on the signs and symptoms of many illnesses that you may come across when working with young children.
There are times when exclusion is the right answer. Licensing states that a child may need to be reasonably separated from other children or sent home if:
- The illness or condition prevents the child from participating in normal activities;
- The illness or condition requires more care and attention than the early learning provider can give;
- The required amount of care for the ill child compromises or places at risk the health and safety of other children in care; or
- There is a risk that the child’s illness or condition will spread to other children or individuals.
Licensing also states that an ill child, staff member, or other individual must be sent home or isolated from children in care (unless they are covered by an individual care plan or protected by the ADA) if the ill individual has:
- A fever 101 degrees Fahrenheit for children over two months (or 100.4 degrees Fahrenheit for an infant younger than two months) by any method, and behavior change or other signs and symptoms of illness (including sore throat, earache, headache, rash, vomiting, diarrhea);
- Vomiting two or more times in the previous twenty-four hours;
- Diarrhea where stool frequency exceeds two stools above normal per twenty-four hours for that child or whose stool contains more than a drop of blood or mucus;
- A rash not associated with heat, diapering, or an allergic reaction;
- Open sores or wounds discharging bodily fluids that cannot be adequately covered with a waterproof dressing or mouth sores with drooling;
- Lice, ringworm, or scabies. Individuals with head lice, ringworm, or scabies must be excluded from the child care premises beginning from the end of the day the head lice, ringworm, or scabies was discovered. The provider may allow an individual with head lice, ringworm, or scabies to return to the premises after receiving the first treatment; or
- A child who appears severely ill, which may include lethargy, persistent crying, difficulty breathing, or a significant change in behavior or activity level indicative of illness.
When a child or staff member has been identified as having a contagious illness, they may not return to the early learning program until they have been assessed by a medical professional and received written remission to return to care. Here is the list of infectious diseases that require immediate removal from the early learning program and a medical provider’s written permission to return to care:
- Bacterial Meningitis
- Haemophilus influenzae invasive disease (excluding Otitis media)
- Meningococcal
- Diarrheal diseases due to or suspected to be caused by an infectious agent
- Cryptosporidiosis
- Giardiasis
- Hepatitis A
- Salmonellosis
- Shigellosis
- Shiga toxin-producing Escherichia coli (STEC)
- Tuberculosis
- Chickenpox (Varicella)
- Diphtheria
- German measles (Rubella)
- Measles (Rubeola)
- Mumps
- Whooping cough (Pertussis)
 |
Danger of Infectious Disease for Adults Because early care and education program employees are around children who are at higher risk of infectious diseases and have limited understanding of hygiene practices, those employees are also at greater risk for getting sick. While most illnesses that are spread in early care and education programs are not serious, some can be very dangerous. Knowledge about illness and how to prevent its spread helps. Being fully immunized (from childhood illness and or vaccines) protects adult health as well. Employees that are or could become pregnant want to be especially careful because first time exposure to chickenpox, cytomegalovirus (CMV), Fifths disease, and Rubella can cause major damage to fetal health, birth defects, and even fetal death.[5] |
Reportable Diseases
Some diseases are enough of a threat to the community that diagnosed cases must be reported to the local health department. If there is an outbreak of any reportable illness (See Table 4.1), a child or staff member who meets the following criteria as determined by the local health department or a health care provider to be:
- contributing to transmission of the illness
- not adequately immunized when the disease is vaccine-preventable
- at increased risk due to the pathogens being circulated.
They can be readmitted when the health department official or that health care provider decides that the risk of transmission is no longer present.[6]
Table 4.1 – Diseases Reportable to Local Health Department (required by Licensing in Washington)[7]
Table HC-1 (Conditions Notifiable by Health Care Providers and Health Care Facilities)
|
Notifiable Condition (Agent) |
Laboratory Confirmation Required Before Submitting Case Report |
Time Frame for Notification from Identification of a Case |
Who Must Be Notified |
Who Must Report: Health Care Providers (Providers) or Health Care Facilities (Facilities) |
|
Acquired immunodeficiency syndrome (AIDS) |
|
Within 3 business days |
DOH (for facilities) and LHJ (for providers) |
Both |
|
Amebic meningitis |
|
Immediately |
LHJ |
Both |
|
Anaplasmosis |
|
Within 3 business days |
LHJ |
Both |
|
Anthrax (Bacillus anthracis and confirmed Bacillus cereus biovar anthracis only – Do not report all Bacillus cereus) |
Yes |
Immediately |
LHJ |
Both |
|
Arboviral disease (acute disease only) including, but not limited to: Chikungunya Dengue Eastern and western equine encephalitis Japanese encephalitis La Crosse encephalitis Powassan virus infection St. Louis encephalitis West Nile virus infection Zika virus infection See also “Yellow fever” |
|
Within 3 business days |
LHJ |
Both |
|
Asthma, occupational |
|
Within 30 days |
Washington state department of labor and industries (L&I) |
Both |
|
Babesiosis |
|
Within 3 business days |
LHJ |
Both |
|
Baylisascariasis |
|
Within 24 hours |
LHJ |
Both |
|
Birth defects – Abdominal wall defects (inclusive of gastroschisis and omphalocele) |
|
Within 30 days |
DOH |
Facilities |
|
Birth defects – Autism spectrum disorders |
|
Within 30 days |
DOH |
Both |
|
Birth defects – Cerebral palsy |
|
Within 30 days |
DOH |
Both |
|
Birth defects – Down syndrome |
|
Within 30 days |
DOH |
Facilities |
|
Birth defects – Alcohol related birth defects |
|
Within 30 days |
DOH |
Both |
|
Birth defects – Hypospadias |
|
Within 30 days |
DOH |
Facilities |
|
Birth defects – Limb reductions |
|
Within 30 days |
DOH |
Facilities |
|
Birth defects – Neural tube defects (inclusive of anencephaly and spina bifida) |
|
Within 30 days |
DOH |
Facilities |
|
Birth defects – Oral clefts (inclusive of cleft lip with/without cleft palate) |
|
Within 30 days |
DOH |
Facilities |
|
Blood lead level RST results (See WAC 246-101-200) |
|
Providers and facilities performing blood lead level RST shall report as a laboratory and comply with the requirements of WAC 246-101-201 through 246-101-230. |
||
|
Botulism, foodborne, infant, and wound |
|
Immediately |
LHJ |
Both |
|
Brucellosis |
|
Within 24 hours |
LHJ |
Both |
|
Campylobacteriosis |
|
Within 3 business days |
LHJ |
Both |
|
Cancer (See chapter 246-102 WAC) |
|
|
|
|
|
Candida auris infection or colonization |
|
Within 24 hours |
LHJ |
Both |
|
Carbapenem-resistant Enterobacteriaceae infections limited to: Klebsiella species E. coli Enterobacter species |
Yes |
Within 3 business days |
LHJ |
Both |
|
Chagas disease |
|
Within 3 business days |
LHJ |
Both |
|
Chancroid |
|
Within 3 business days |
LHJ |
Both |
|
Chlamydia trachomatis infection |
Yes |
Within 3 business days |
LHJ |
Both |
|
Cholera (Vibrio cholerae O1 or O139) |
Yes |
Immediately |
LHJ |
Both |
|
Coccidioidomycosis |
|
Within 3 business days |
LHJ |
Both |
|
Coronavirus infection (severe communicable) SARS-associated coronavirus MERS-associated coronavirus Novel coronavirus (COVID-19) |
Yes |
Immediately |
LHJ |
Both |
|
Coronavirus infection (severe communicable) Novel coronavirus (COVID-19) RST results (See WAC 246-101-200) |
|
Providers and facilities performing Novel coronavirus (COVID-19) RST shall report as a laboratory and comply with the requirements of WAC 246-101-201 through 246-101-230. |
||
|
Cryptococcus gattii or undifferentiated Cryptococcus species (i.e., Cryptococcus not identified as C. neoformans) |
Yes |
Within 3 business days |
LHJ |
Both |
|
Cryptosporidiosis |
|
Within 3 business days |
LHJ |
Both |
|
Cyclosporiasis |
|
Within 3 business days |
LHJ |
Both |
|
Cysticercosis |
|
Within 3 business days |
LHJ |
Both |
|
Diphtheria |
|
Immediately |
LHJ |
Both |
|
Domoic acid poisoning |
|
Immediately |
LHJ |
Both |
|
E. coli (See “Shiga toxin-producing E. coli”) |
|
|
|
|
|
Echinococcosis |
|
Within 3 business days |
LHJ |
Both |
|
Ehrlichiosis |
|
Within 3 business days |
LHJ |
Both |
|
Giardiasis |
|
Within 3 business days |
LHJ |
Both |
|
Glanders (Burkholderia mallei) |
Yes |
Immediately |
LHJ |
Both |
|
Gonorrhea |
|
Within 3 business days |
LHJ |
Both |
|
Granuloma inguinale |
|
Within 3 business days |
LHJ |
Both |
|
Gunshot wounds (nonfatal) |
|
Within 30 days |
DOH |
Facilities |
|
Haemophilus influenzae (invasive disease, children under 5 years of age) |
Yes |
Immediately |
LHJ |
Both |
|
Hantaviral infection |
|
Within 24 hours |
LHJ |
Both |
|
Hepatitis A (acute infection) |
Yes |
Within 24 hours |
LHJ |
Both |
|
Hepatitis B (acute infection) |
Yes |
Within 24 hours |
LHJ |
Both |
|
Hepatitis B, report pregnancy in hepatitis B virus infected patients (including carriers) |
Yes |
Within 3 business days |
LHJ |
Both |
|
Hepatitis B (chronic infection) – Initial diagnosis, and previously unreported prevalent cases |
Yes |
Within 3 business days |
LHJ |
Both |
|
Hepatitis B (perinatal) – Initial diagnosis, and previously unreported cases |
Yes |
Within 3 business days |
LHJ |
Both |
|
Hepatitis C (acute infection) |
Yes |
Within 24 hours |
LHJ |
Both |
|
Hepatitis C (acute infection) RST results (See WAC 246-101-200) |
|
Providers and facilities performing hepatitis C (acute infection) RST shall report as a laboratory and comply with the requirements of WAC 246-101-201 through 246-101-230. |
||
|
Hepatitis C (chronic infection) |
Yes |
Within 3 business days |
LHJ |
Both |
|
Hepatitis C (perinatal) – Initial diagnosis, and previously unreported cases |
Yes |
Within 24 hours |
LHJ |
Both |
|
Hepatitis C (chronic infection) RST results (See WAC 246-101-200) |
|
Providers and facilities performing hepatitis C (chronic infection) RST shall report as a laboratory and comply with the requirements of WAC 246-101-201 through 246-101-230. |
||
|
Hepatitis D (acute and chronic infection) |
Yes |
Within 24 hours |
LHJ |
Both |
|
Hepatitis E (acute infection) |
Yes |
Within 24 hours |
LHJ |
Both |
|
Herpes simplex, neonatal and genital (initial infection only) |
|
Within 3 business days |
LHJ |
Providers |
|
Histoplasmosis |
|
Within 3 business days |
LHJ |
Both |
|
Human immunodeficiency virus (HIV) infection |
|
Within 3 business days |
LHJ |
Both |
|
Human immunodeficiency virus (HIV) infection RST results (See WAC 246-101-200) |
|
Providers and facilities performing HIV infection RST shall report as a laboratory and comply with the requirements of WAC 246-101-201 through 246-101-230. |
||
|
Human prion disease |
|
Within 3 business days |
LHJ |
Both |
|
Hypersensitivity pneumonitis, occupational |
|
Within 30 days |
L&I |
Both |
|
Influenza, novel or unsubtypable strain |
|
Immediately |
LHJ |
Both |
|
Influenza-associated death (laboratory confirmed) |
Yes |
Within 3 business days |
LHJ |
Both |
|
Legionellosis |
|
Within 24 hours |
LHJ |
Both |
|
Leptospirosis |
|
Within 24 hours |
LHJ |
Both |
|
Listeriosis |
|
Within 24 hours |
LHJ |
Both |
|
Lyme disease |
|
Within 3 business days |
LHJ |
Both |
|
Lymphogranuloma venereum |
|
Within 3 business days |
LHJ |
Both |
|
Malaria |
|
Within 3 business days |
LHJ |
Both |
|
Measles (rubeola) – Acute disease only |
|
Immediately |
LHJ |
Both |
|
Melioidosis (Burkholderia pseudomallei) |
Yes |
Immediately |
LHJ |
Both |
|
Meningococcal disease, invasive |
|
Immediately |
LHJ |
Both |
|
Monkeypox |
|
Immediately |
LHJ |
Both |
|
Mumps, acute disease only |
|
Within 24 hours |
LHJ |
Both |
|
Outbreaks and suspected outbreaks |
|
Immediately |
LHJ |
Both |
|
Paralytic shellfish poisoning |
|
Immediately |
LHJ |
Both |
|
Pertussis |
|
Within 24 hours |
LHJ |
Both |
|
Pesticide poisoning (hospitalized, fatal, or cluster) |
|
Immediately |
DOH |
Both |
|
Pesticide poisoning (all other) |
|
Within 3 business days |
DOH |
Both |
|
Plague |
|
Immediately |
LHJ |
Both |
|
Poliomyelitis |
|
Immediately |
LHJ |
Both |
|
Pregnancy in patient with hepatitis B virus |
|
See “Hepatitis B, report pregnancy in hepatitis B virus infected patients (including carriers)” |
||
|
Psittacosis |
|
Within 24 hours |
LHJ |
Both |
|
Q fever |
|
Within 24 hours |
LHJ |
Both |
|
Rabies (suspect or laboratory confirmed human cases and laboratory confirmed animal cases) |
Yes for animal cases |
Immediately |
LHJ |
Both |
|
Rabies, suspected human exposure (suspected human rabies exposures due to a bite from or other exposure to an animal that is suspected of being infected with rabies) |
|
Immediately |
LHJ |
Both |
|
Relapsing fever (borreliosis) |
|
Within 3 business days |
LHJ |
Both |
|
Rickettsia infection |
|
Within 3 business days |
LHJ |
Both |
|
Rubella, acute disease only (including congenital rubella syndrome) |
|
Immediately |
LHJ |
Both |
|
Salmonellosis |
|
Within 24 hours |
LHJ |
Both |
|
Serious adverse reactions to immunizations |
|
Within 3 business days |
LHJ |
Both |
|
Shiga toxin-producing E. coli (STEC) infections/enterohemorrhagic E. coli infections |
Yes |
Immediately |
LHJ |
Both |
|
Shigellosis |
|
Within 24 hours |
LHJ |
Both |
|
Silicosis |
|
Within 30 days |
L&I |
Both |
|
Smallpox |
|
Immediately |
LHJ |
Both |
|
Syphilis |
|
Within 3 business days |
LHJ |
Both |
|
Taeniasis |
|
Within 3 business days |
LHJ |
Both |
|
Tetanus |
|
Within 3 business days |
LHJ |
Both |
|
Tick paralysis |
|
Within 3 business days |
LHJ |
Both |
|
Trichinosis |
|
Within 3 business days |
LHJ |
Both |
|
Tuberculosis disease (confirmed or highly suspicious, i.e., initiation of empiric treatment) |
|
Within 24 hours |
LHJ |
Both |
|
Tularemia |
|
Immediately |
LHJ |
Both |
|
Typhus |
|
Within 3 business days |
LHJ |
Both |
|
Vaccinia transmission |
|
Immediately |
LHJ |
Both |
|
Vancomycin-resistant Staphylococcus aureus (not to include vancomycin-intermediate) |
Yes |
Within 24 hours |
LHJ |
Both |
|
Varicella-associated death |
|
Within 3 business days |
LHJ |
Both |
|
Vibriosis (Vibrio species not including Vibrio cholerae O1 or O139) See Cholera (Vibrio cholerae O1 or O139) |
Yes |
Within 24 hours |
LHJ |
Both |
|
Viral hemorrhagic fever |
|
Immediately |
LHJ |
Both |
|
Yellow fever |
|
Immediately |
LHJ |
Both |
|
Yersiniosis |
|
Within 24 hours |
LHJ |
Both |
|
Unexplained critical illness or death |
|
Within 24 hours |
LHJ |
Both |
 |
Reflective Practice Consider the following situations. Should each child be excluded from care or not? If so, why and when should the child return? If not, what should the teacher/caregiver do? Mario’s dad drops him off and let’s Ms. Michelle know that he is a little under the weather. He is not running a fever, but has a mild cough and a runny nose. But he ate a good breakfast and has a pretty typical level of energy. About an hour into the day, Li vomits. Mr. Abraham checks and she has a fever of 101.3°. She looks a little pale and just wants to lay down. As he goes to call Li’s family, she vomits again. When Latanya goes to change Daniel’s diaper she notices a rash on his stomach. She checks his temperature and he is not running a fever. He is not scratching at it or seemingly in any discomfort. She remembers that he has a history of eczema and contact dermatitis. Apurva wakes up from naptime with discharge coming from a slightly swollen and bloodshot right eye. She tells Ms. Maria that her eye hurts and is “kind of itchy.” Now, come up with your own examples of a child that should be excluded from care and that should not automatically be excluded. |
Caring for Mildly Ill Children
Because young children in early care and education programs have a high incidence of illness and may have ongoing medical conditions (such as eczema and asthma), providers should be prepared to care for mildly ill children, at least temporarily. And since we know that excluding most mildly ill children doesn’t prevent the spread of illness and can have negative effects on families, programs should consider whether they can care for children with mild symptoms (not meeting the exclusion policy). The California Childcare Health Program poses the following questions to consider:
- Are there sufficient staff (including volunteers) to provide minor modifications that a child might need (such as quiet activities or extra fluids)?
- Are staff willing and able to care for the child’s symptoms (such as wiping a runny nose and checking a fever) without neglecting the care of other children in the group?
- Is there a space where the mildly ill child can rest if needed?
- Are families able or willing to pay extra for sick care if other resources are not available, so that you can hire extra staff as needed?
- Have families made alternative arrangements for someone to pick up and care for their ill children if they cannot?
It’s important that programs recognize the families have to weigh many things when trying to decide whether or not to send a child to child care. They must consider how the child feels (physically and emotionally) whether or not the program can provide care for the specific needs of the child, what alternative care arrangements are available, as well as the income they may lose if they have to stay home.[8]
|
Responding to Illness that Requires Medical Care
Some conditions require immediate medical help. If the parents can be reached, tell them to come right away and to notify their medical provider. Call Emergency Medical services (9-1-1) immediately and also notify parents if any of the following things happen:
Tell the parent to come right away, and get medical help immediately, when any of the following things happen. If the parent or the child’s medical provider is not immediately available, call 9-1-1 (EMS) for immediate help:
|
Administering Medications
Some children in your early care and education setting may need to take medications during the hours you provide care for them. It’s important that early care and education programs have a written policy for the use of prescription and nonprescription medication.[10]
According to licensing, programs that choose to handle medications must abide by the following:

- All prescription and nonprescription medications shall be centrally stored in a safe place inaccessible to children, with an unaltered label, and labeled with the child’s name and date
- A refrigerator shall be used to store any medication that requires refrigeration.
- Prescription medications may be administered with written permission by the child’s authorized representatives in accordance with the label instructions by the physician
- Nonprescription medications may be administered without approval or instructions from the child’s physician with written approval and instructions from the child’s authorized representative and when administered in accordance with the product label directions.
Valid reasons for an early care and education program to consider administering medication:
- Some medication dosing cannot be adjusted to be taken before and after care (and keeping them out of care when otherwise well enough to attend, would be a hardship for families.
- Some children may have chronic conditions that may require urgent administration of medication (such as asthma and diabetes).[11]
Communication with Families
When children are excluded from care, it’s important to provide documentation for families of how the child meets the guidelines in your exclusion policy and what needs to happen before the child can return to care. Programs are also required to inform families when children are exposed to a communicable disease.
|
Reflective Practice Why is it important for early care and education programs to communicate clearly with families regarding communicable illness? |
Summary
Becoming familiar with infectious diseases that are common in early childhood enables early care and education program staff to identify illness and respond appropriately. This included knowing when children (and staff) should be excluded from care and what needs to happen before they should come back.
Programs must create policies on how they will handle children that are mildly ill (those that need care before they can be picked up from care and those that do not require exclusion) and children who have illness that requires medical care. Programs who choose to administer medication, must be familiar with the licensing regulations they must follow.
Open communication with families is important when a child becomes ill or is potentially exposed to an illness. Helping families understand and follow policies regarding exclusion is vital to keeping everyone in the program as healthy as possible.
 |
Resources for Further Exploration |
- WAC 110-300-0205.pdf (SECURED) ↵
- https://app.leg.wa.gov/WAC/default.aspx?cite=246-110 ↵
- Infectious Diseases: Prevention and Management by Head Start Early Childhood Learning & Knowledge Center is in the public domainhttps://eclkc.ohs.acf.hhs.gov/physical-health/article/infectious-diseases-prevention-management ↵
- California Childcare Health Program. (2018). Preventive Health and Safety in the Child Care Setting: A Curriculum for the Training of Child Care Providers (3rd ed.). University of California, San Francisco. Retrieved from https://cchp.ucsf.edu/sites/g/files/tkssra181/f/PHT-Handbook-Student-2018-FINAL.pdf ↵
- California Child Care Health Program. (2011). Health and Safety in the Child Care Setting: Prevention of Infectious Disease. University of California San Francisco. Retrieved from https://cchp.ucsf.edu/sites/g/files/tkssra181/f/idc2book.pdf ↵
- Infectious Disease Outbreak Control by Head Start Early Childhood Learning & Knowledge Center is in the public domain ↵
- https://app.leg.wa.gov/WAC/default.aspx?cite=246-101-101 ↵
- California Childcare Health Program. (2018). Preventive Health and Safety in the Child Care Setting: A Curriculum for the Training of Child Care Providers (3rd ed.). University of California, San Francisco. Retrieved from https://cchp.ucsf.edu/sites/g/files/tkssra181/f/PHT-Handbook-Student-2018-FINAL.pdf ↵
- California Childcare Health Program. (2018). Preventive Health and Safety in the Child Care Setting: A Curriculum for the Training of Child Care Providers (3rd ed.). University of California, San Francisco. Retrieved from https://cchp.ucsf.edu/sites/g/files/tkssra181/f/PHT-Handbook-Student-2018-FINAL.pdf ↵
- California Childcare Health Program. (2018). Preventive Health and Safety in the Child Care Setting: A Curriculum for the Training of Child Care Providers (3rd ed.). University of California, San Francisco. Retrieved from https://cchp.ucsf.edu/sites/g/files/tkssra181/f/PHT-Handbook-Student-2018-FINAL.pdf ↵
- California Childcare Health Program. (2018). Preventive Health and Safety in the Child Care Setting: A Curriculum for the Training of Child Care Providers (3rd ed.). University of California, San Francisco. Retrieved from https://cchp.ucsf.edu/sites/g/files/tkssra181/f/PHT-Handbook-Student-2018-FINAL.pdf ↵
