8
Chapter 8: Sexual Response and the Biochemistry of Love
Learning Outcomes:
- Consider intersectionality as it applies to individual’s sexual responses
- Explore the role of brain and hormonal mechanisms in sexual response, as well as sensation & perception
- Distinguish between hormones and pheromones
- Describe the seminal work of Master’s & Johnson’s EPOR model of sexual response
- Compare other theories of sexual response, including Kaplan, Basson & the Dual Control approach
- Analyze the concept of love with emerging research on evolution & physiology
- Explore the importance of oxytocin in social interactions
Introduction
If you remember (or go back and revisit) the “Circles of Sexuality” model from Chapter 1, you will see that sensuality plays a key role in our sexuality. Sensuality is also interconnected with intimacy, sexual identity, sexual health and reproduction, and sexualization. Let’s take a closer look at the sensual aspect of sexuality by analyzing physiological responses while also seeing the whole picture in which many interlocking parts are influencing the way individuals make meaning out of their physical, bodily experiences. The changes to brain chemistry, the hormones that rush through the bloodstream, the sensory neurons behind that electric and tingling feeling of intimate touch, the role of erogenous zones in enhancing pleasure, and the pheromones that we put off that are picked up without conscious awareness by others will be explored. The psychological interpretation of the physical changes that are happening during arousal and orgasm are also influenced by society, culture, and personal perspective that can alter the way that meaning is made out of these experiences. The biochemistry of love will be discussed in which heartbreak and the epigenetic and healing effects of oxytocin will be explored.
Sexual Response
Sexual response is both biological and based on socialization factors. Each individual person has a natural degree to which they become aroused in response to sexual stimuli similar to how some people react more intensely to loud sounds or have a low to high pain tolerance. Life experiences across the lifespan continue to influence and change these as well. Individual differences in how sexual stimuli are experienced will influence the degree of desire to engage in certain sexual behaviors. Social factors, such as shame and stigma around certain sexual behaviors, can also influence this process by reworking the way that touch and sexual contact are perceived. In this section, we will look at different aspects of the nervous system that are implicated in this process, explore the groundbreaking Masters and Johnson research on the sexual response cycle, and discuss additional theories that have been developed over time that explore the ways the social environment interacts with sensory experiences.
Sex on the Brain

Figure 3: Some of the many regions of the brain and brainstem activated during pleasure experiences. [Image: Frank Gaillard, https://goo.gl/yCKuQ2, CC-BY-SA 3.0. Identifying marks added]
At first glance—or touch for that matter—the clitoris and penis are the parts of our anatomies that seem to bring the most pleasure. However, these two organs pale in comparison to our central nervous system’s capacity for pleasure. Extensive regions of the brain and brainstem are activated when a person experiences pleasure, including: the insula, temporal cortex, limbic system, nucleus accumbens, basal ganglia, superior parietal cortex, dorsolateral prefrontal cortex, and cerebellum (see Figure 3, Ortigue et al., 2007). Neuroimaging techniques show that these regions of the brain are active when patients have spontaneous orgasms involving no direct stimulation of the skin (e.g., Fadul et al., 2005) and when experimental participants self-stimulate erogenous zones (e.g., Komisaruk et al., 2011). Erogenous zones are sensitive areas of skin that are connected, via the nervous system, to the somatosensory cortex in the brain.
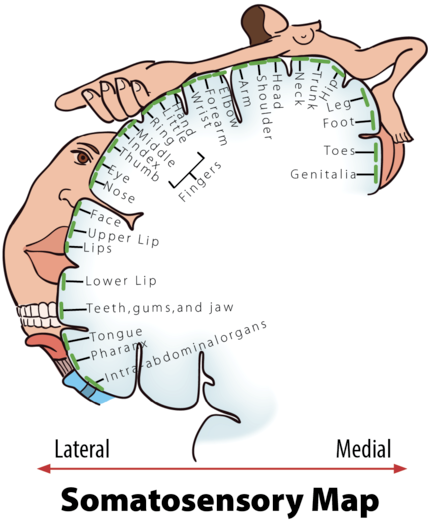
Figure 4: Erogenous Zones Mapped on the Somatosensory Cortex.
The somatosensory cortex (SC) is the part of the brain primarily responsible for processing sensory information from the skin. The more sensitive an area of your skin is (e.g., your lips), the larger the corresponding area of the SC will be; the less sensitive an area of your skin is (e.g., your trunk), the smaller the corresponding area of the SC will be (see Figure 4, Penfield & Boldrey, 1937). When a sensitive area of a person’s body is touched, it is typically interpreted by the brain in one of three ways: “That tickles!” “That hurts!” or, “That…you need to do again!” Thus, the more sensitive areas of our bodies have greater potential to evoke pleasure. A study by Nummenmaa and his colleagues (2016) used a unique method to test this hypothesis. The Nummenmaa research team showed experimental participants images of same- and opposite-sex bodies. They then asked the participants to color the regions of the body that, when touched, they or members of the opposite sex would experience as sexually arousing while masturbating or having sex with a partner. Nummenmaa found the expected “hotspot” erogenous zones around the external sex organs, breasts, and anus, but also reported areas of the skin beyond these hotspots: “[T]actile stimulation of practically all bodily regions trigger sexual arousal….” Moreover, he concluded, “[H]aving sex with a partner…”—beyond the hotspots—“…reflects the role of touching in the maintenance of…pair bonds.”
Sensation and Perception
Sensation is the way the nervous system, such as different areas of the brain, processes sensory information from the environment, such as light, sound, smell, and touch/pain. Let’s take a look at touch in the context of sensual contact by explaining the process of transduction–receptors in the skin relay the message of being touched to transmitters in the spinal cord that converts this to neural signals interpreted by the brain which then allows effectors, neurons within muscles, to signal a response to the stimuli, such as by jerking away the hand when something is hot. Perception is how an individual associates meaning with what they are sensing. For instance, masturbation will cause the genital’s skin receptor sites and nervous system to respond to this sensation producing arousal; however, the self-talk regarding the morality of masturbation will impact the way the person perceives the arousal. Pay attention to the way that stigma and shame around pleasure and sensuality have influenced the way you attach meaning to your physiological experiences.
Exploring your erogenous zones: What areas of your body feel particularly pleasurable to the touch? Some common areas, apart from the genitals, are the lower back, inner thighs, lips, nipples, feet, hands, and more! Each individual will have specific areas so explore this question with your sexual partners as well.
Sensate focus is sometimes utilized within sex therapy to increase control over physiological responses and to provide insight into sexual partners’ pleasure points in addition to one’s own without touching or stimulating the genitals. Anxiety is experienced by many individuals as being sensual can feel very vulnerable and scary. Sensate focus uses aspects of cognitive-behavioral therapy and behavioral modification to focus on the senses and alter the meaning that has been associated with sexual interactions. Check out this article on sensate focus techniques from Cornell University (2019). These techniques can be utilized by anyone who is interested and can enhance sexual pleasure through increasing self-awareness and communication focused on pleasure with partners.
Hormones and Pheromones
Androgens, estrogen, and progestin bind to hormone receptor sites that allow the synthesis of neurochemicals (Hyde & DeLamater, 2017). During excitement and arousal, dopamine, oxytocin, and norepinephrine are released into the bloodstream, and during orgasm, opioids and endocannabinoids are released (Hyde & DeLamater, 2017). Hormones have activating effects in which they can activate and deactivate sexual arousal. Testosterone is particularly implicated in increasing desire for sex. Too high or too low of testosterone reduces desire. Intense emotions increase sexual arousal such as happiness, anger, anxiety, sadness, etc. because of their physiological impacts on our endocrine and nervous systems. For instance, sex and aggression both involve the hormones epinephrine and norepinephrine (which are also neurotransmitters) as they invoke a sense of excitement then resolution. This connection between emotions and our physiological reactions is a growing focus within research (Hyde & DeLamater, 2017).
While hormones are typically released within the bloodstream and influence sexual arousal, pheromones are biochemicals secreted outside the body that communicate to others on a chemical level about hormonal levels and ovulation which subconsciously attracts us to them based on our own body’s chemistry (Hyde & DeLamater, 2017). Researchers are still trying to understand the role of pheromones in sexual responses, but what is known is that when people are presented with the scent of others they are typically more attracted to the smell of someone in a way that matches with their sexual orientation even without any other information provided (Savic, 2014). Additionally, the scent of people who are biologically related is rated as less attractive and possibly connects to evolution protecting against unintentional incest (Savic, 2014). Animal studies on male monkeys indicate that they experience increases in testosterone when exposed to an ovulating female’s urine (Hyde & DeLamater, 2017). Pheromones are believed to influence the hormones in others and this can be seen by women’s menstrual cycles syncing up when they spend a lot of time with each other as well. This further showcases how interconnected humans are with one another biologically in addition to socially.
Theories and Models Regarding Sexual Response
Masters and Johnson
Although people have always had sex, the scientific study of it has remained taboo until relatively recently. In fact, the study of sexual anatomy, physiology, and behavior wasn’t formally undertaken until the late 19th century, and only began to be taken seriously as recently as the 1950’s. Notably, William Masters (1915-2001) and Virginia Johnson (1925-2013) formed a research team in 1957 that expanded studies of sexuality from merely asking people about their sex lives to measuring people’s anatomy and physiology while they were actually having sex. Masters was a former Navy lieutenant, married father of two, and trained gynecologist with an interest in studying prostitutes. Johnson was a former country music singer, single mother of two, three-time divorcee, and two-time college dropout with an interest in studying sociology. And yes, if it piques your curiosity, Masters and Johnson were lovers (when Masters was still married); they eventually married each other, but later divorced. Despite their colorful private lives they were dedicated researchers with an interest in understanding sex from a scientific perspective.
Masters and Johnson used primarily plethysmography (the measuring of changes in blood- or airflow to organs) to determine sexual responses in a wide range of body parts—breasts, skin, various muscle structures, bladder, rectum, external sex organs, and lungs—as well as measurements of people’s pulse and blood pressure. They measured more than 10,000 orgasms in 700 individuals (18 to 89 years of age), during sex with partners or alone. Masters and Johnson’s findings were initially published in two best-selling books: Human Sexual Response, 1966, and Human Sexual Inadequacy, 1970. Their initial experimental techniques and data form the bases of our contemporary understanding of sexual anatomy and physiology.
Physiology and the Sexual Response Cycle
The brain and other sex organs respond to sexual stimuli in a universal fashion known as the sexual response cycle (SRC; Masters & Johnson, 1966). The SRC is composed of four phases:
- Excitement: Activation of the sympathetic branch of the autonomic nervous system defines the excitement phase; heart rate and breathing accelerates, along with increased blood flow to the penis, vaginal walls, clitoris, and nipples (vasocongestion). Involuntary muscular movements (myotonia), such as facial grimaces, also occur during this phase.
- Plateau: Blood flow, heart rate, and breathing intensify during the plateau phase. During this phase, often referred to as “foreplay,” females experience an orgasmic platform—the outer third of the vaginal walls tightening—and males experience a release of pre-seminal fluid containing healthy sperm cells (Killick et al., 2011). This early release of fluid makes penile withdrawal a relatively ineffective form of birth control (Aisch & Marsh, 2014). (Question: What do you call a couple who use the withdrawal method of birth control? Answer: Parents.)
- Orgasm: The shortest but most pleasurable phase is the orgasm phase. After reaching its climax, neuromuscular tension is released and the hormone oxytocin floods the bloodstream—facilitating emotional bonding. Although the rhythmic muscular contractions of an orgasm are temporally associated with ejaculation, this association is not necessary because orgasm and ejaculation are two separate physiological processes.
- Resolution: The body returns to a pre-aroused state in the resolution phase. Most males enter a refractory period of being unresponsive to sexual stimuli. The length of this period depends on age, frequency of recent sexual relations, level of intimacy with a partner, and novelty. Because most females do not have a refractory period, they have a greater potential—physiologically—of having multiple orgasms.
Of interest to note, the SRC occurs regardless of the type of sexual behavior—whether the behavior is masturbation; romantic kissing; or oral, vaginal, or anal sex (Masters & Johnson, 1966). Further, a partner or environmental object is sufficient, but not necessary, for the SRC to occur.
Kaplan’s Triphasic Model
Helen Singer Kaplan was a sex therapist seeking a model that would aid her in explaining the sexual response cycle to her clients. Kaplan adjusted Masters and Johnsons’ model by adding the desire phase and reduced excitement and plateau to just the excitement phase in which she focused on vasocongestion occurring. By focusing on the psychological and physiological processes more than trying to separate these experiences, her model became:
- Desire: Desire activates excitement and excitement can cause desire, motivating a person toward sexual activity. This phase is psychological while the next two are physiological.
- Arousal: Vasocongestion causes blood to flow to the genitals and increase in blood pressure and is controlled by the parasympathetic division of the autonomic nervous system (Hyde & DeLamater, 2017, p. 191)
- Orgasm: Reflex muscular contractions also involve anatomical structures and are connected to the nervous system. The ejaculation reflex can be controlled whereas the erection reflex typically cannot. Ejaculation and orgasm are controlled by the sympathetic division of the autonomic nervous system in order to return the body to homeostasis.
Unfortunately, Kaplan’s model did not seem to reflect women’s experience (Lieblum, 2000). Many women never experience spontaneous desire and for those who do, it does not always lead to sexual engagement or arousal. Furthermore, for many people, arousal occurs before desire. Finally, Kaplan’s model didn’t address sexual satisfaction (though her clinical work was built on that).
Basson’s Nonlinear Approach to Sexual Response
In response to to Masters & Johnson, linear model (where there is a start, a middle, and a finish line) and Kaplan’s incomplete model, Rosemary Basson articulated a more complex, circular model of sexual response. Basson’s circular diagram shows how sex is cyclical: desire often comes in response to something else, like a touch or an erotic conversation. If the sex is hot, even the fading memory of it could become motivation for more sex/arousal later on. Finally, sexual encounters don’t have to end with a mutual orgasm. They end with satisfaction, however a couple defines that, whether that’s five orgasms or none.
While this model was first conceptualized with female sexuality in mind, it’s applicable to all.
The Dual Control Model
This model was developed by former Kinsey Institute director Dr. John Bancroft and Dr. Erick Janssen in the late 1990s. It “proposes that two basic processes underlie human sexual response: excitation (responding with arousal to sexual stimuli) and inhibition (inhibiting sexual arousal)” (Hyde & DeLamater, 2017, p. 191). We have evolutionarily developed an inhibition aspect to the sexual response process to protect us from dying. Imagine you are in the middle of having sex and a dinosaur begins to run at you. Survival requires the ability to inhibit sexual arousal to focus on getting away to safety. Or, perhaps a more realistic example could be masturbating in the privacy of a bedroom when there is a sudden knock on the door and mom saying she is coming in. Mom is not a dinosaur but she is going to have that same inhibiting impact.
This perspective also explores the reason why some people may be more easily aroused by sexual stimuli while others may be less impacted. Every person has their own degree of excitation and inhibition similar to how each person has different tolerances for loud sounds or pain. If a person has high excitation and low inhibition, it may be easier for them to become aroused and take more time to return to homeostasis. Touch and sensations may be heightened and they may require less stimulation to reach orgasm. On the other hand, if someone has low excitation and high inhibition, sexual stimuli may be less arousing and they may require a broader range of sensual stimulation to achieve orgasm. Excitation and inhibition are negatively correlated with one another because as one increases the other decreases.
We are genetically predisposed to having a certain combination of sexual excitation and inhibition. However, the dual control model also recognizes that there are cognitive factors shaping this process. Our experiences impact the interpretation of the senses and can cause heightened distress or increased tolerance. Early learning and culture can then drastically shape someone’s excitation and inhibition combination. Many researchers liken it to having both a gas pedal (excitation or SES) and a brake pedal (inhibition or SIS) in a car – people will often engage one or both pedals to a differing degree in any particular sexual situation, depending on their unique sexual physiology, history, and personality.
In thinking about intersecting identities, how could generation, physical health, mental health, religion, education, family background, financial resources, body image, and more influence excitation and inhibition? What messages about various sexual behaviors have you internalized, and how might this influence your neurological sexual response? Having a conversation with your partners about their degree of excitation and inhibition can be helpful to know in relation to your own as well.
The Biochemistry of Love
Love is deeply biological. It pervades every aspect of our lives and has inspired countless works of art. Love also has a profound effect on our mental and physical state. A “broken heart” or a failed relationship can have disastrous effects; bereavement disrupts human physiology and may even precipitate death. Without loving relationships, humans fail to flourish, even if all of their other basic needs are met. As such, love is clearly not “just” an emotion; it is a biological process that is both dynamic and bidirectional in several dimensions. Social interactions between individuals, for example, trigger cognitive and physiological processes that influence emotional and mental states. In turn, these changes influence future social interactions. Similarly, the maintenance of loving relationships requires constant feedback through sensory and cognitive systems; the body seeks love and responds constantly to interactions with loved ones or to the absence of such interactions. The evolutionary principles and ancient hormonal and neural systems that support the beneficial and healing effects of loving relationships are described here.
Introduction to the Study of Love
Although evidence exists for the healing power of love, only recently has science turned its attention to providing a physiological explanation for love. The study of love in this context offers insight into many important topics, including the biological basis of interpersonal relationships and why and how disruptions in social bonds have such pervasive consequences for behavior and physiology. Some of the answers will be found in our growing knowledge of the neurobiological and endocrinological mechanisms of social behavior and interpersonal engagement.
The evolution of social behavior
Nothing in biology makes sense except in the light of evolution. Life on earth is fundamentally social: The ability to dynamically interact with other living organisms to support mutual homeostasis, growth, and reproduction evolved very early. Social interactions are present in primitive invertebrates and even among prokaryotes: Bacteria recognize and approach members of their own species. Bacteria also reproduce more successfully in the presence of their own kind and are able to form communities with physical and chemical characteristics that go far beyond the capabilities of the individual cell (Ingham & Ben-Jacob, 2008).
The evolutionary pathways that led from reptiles to mammals allowed the emergence of the unique anatomical systems and biochemical mechanisms that enable social engagement and selectively reciprocal sociality. Reptiles show minimal parental investment in offspring and form nonselective relationships between individuals. Pet owners may become emotionally attached to their turtle or snake, but this relationship is not reciprocal. In contrast, most mammals show intense parental investment in offspring and form lasting bonds with their children. Many mammalian species—including humans, wolves, and prairie voles—also develop long-lasting, reciprocal, and selective relationships between adults, with several features of what humans experience as “love.” In turn, these reciprocal interactions trigger dynamic feedback mechanisms that foster growth and health.
What is love? An evolutionary and physiological perspective
Human love is more complex than simple feedback mechanisms. Love may create its own reality. The biology of love originates in the primitive parts of the brain—the emotional core of the human nervous system—which evolved long before the cerebral cortex. The brain “in love” is flooded with vague sensations, often transmitted by the vagus nerve, and creating much of what we experience as emotion. The modern cortex struggles to interpret love’s messages, and weaves a narrative around incoming visceral experiences, potentially reacting to that narrative rather than to reality. It also is helpful to realize that mammalian social behavior is supported by biological components that were repurposed or co-opted over the course of mammalian evolution, eventually permitting lasting relationships between adults.
Stress and love
Emotional bonds can form during periods of extreme duress, especially when the survival of one individual depends on the presence and support of another. There also is evidence that oxytocin is released in response to acutely stressful experiences, perhaps serving as hormonal “insurance” against overwhelming stress. Oxytocin may help to ensure that parents and others will engage with and care for infants; develop stable, loving relationships; and seek out and receive support from others in times of need.
The absence of love in early life can be detrimental to mental and physical health
During early life in particular, trauma or neglect may produce behaviors and emotional states in humans that are socially pathological. Because the processes involved in creating social behaviors and social emotions are delicately balanced, these be may be triggered in inappropriate contexts, leading to aggression toward friends or family. Alternatively, bonds may be formed with prospective partners who fail to provide social support or protection.
Loving relationships in early life can have epigenetic consequences
Love is “epigenetic.” That is, positive experiences in early life can act upon and alter the expression of specific genes. These changes in gene expression may have behavioral consequences through simple biochemical changes, such as adding a methyl group to a particular site within the genome (Zhang & Meaney, 2010). It is possible that these changes in the genome may even be passed to the next generation.
Although we are all born with a finite set of genes, experiences in childhood will cause some genes to express themselves (e.g., encourage certain personality traits), while other genes will remain dormant.
Social behaviors, emotional attachment to others, and long-lasting reciprocal relationships also are both plastic and adaptive, and so is the biology upon which they are based. For example, infants of traumatized or highly stressed parents might be chronically exposed to vasopressin, either through their own increased production of the peptide, or through higher levels of vasopressin in maternal milk. Such increased exposure could sensitize the infant to defensive behaviors or create a lifelong tendency to overreact to threat. Based on research in rats, it seems that in response to adverse early experiences of chronic isolation, the genes for vasopressin receptors can become upregulated (Zhang et al., 2012), leading to an increased sensitivity to acute stressors or anxiety that may persist throughout life.
Epigenetic programming triggered by early life experiences is adaptive in allowing neuroendocrine systems to project and plan for future behavioral demands. But epigenetic changes that are long-lasting also can create atypical social or emotional behaviors (Zhang & Meaney, 2010) that may be especially likely to surface in later life, and in the face of social or emotional challenges.
Exposure to exogenous hormones in early life also may be epigenetic. For example, prairie voles treated postnatally with vasopressin (especially males) were later more aggressive, whereas those exposed to a vasopressin antagonist showed less aggression in adulthood. Conversely, in voles the exposure of infants to slightly increased levels of oxytocin during development increased the tendency to show a pair bond. However, these studies also showed that a single exposure to a higher level of oxytocin in early life could disrupt the later capacity to pair bond (Carter et al., 2009).
There is little doubt that either early social experiences or the effects of developmental exposure to these neuropeptides holds the potential to have long-lasting effects on behavior. Both parental care and exposure to oxytocin in early life can permanently modify hormonal systems, altering the capacity to form relationships and influence the expression of love across the life span. Our preliminary findings in voles further suggest that early life experiences affect the methylation of the oxytocin receptor gene and its expression (Connelly, Kenkel, Erickson, & Carter, 2011). Thus, we can plausibly argue that love is epigenetic.
The absence of social behavior or isolation also has consequences for the oxytocin system
Given the power of positive social experiences, it is not surprising that a lack of social relationships also may lead to alterations in behavior as well as changes in oxytocin and vasopressin pathways. We have found that social isolation reduced the expression of the gene for the oxytocin receptor, and at the same time increased the expression of genes for the vasopressin peptide. In female prairie voles, isolation also was accompanied by an increase in blood levels of oxytocin, possibly as a coping mechanism. However, over time, isolated prairie voles of both sexes showed increases in measures of depression, anxiety, and physiological arousal, and these changes were observed even when endogenous oxytocin was elevated. Thus, even the hormonal insurance provided by endogenous oxytocin in face of the chronic stress of isolation was not sufficient to dampen the consequences of living alone. Predictably, when isolated voles were given additional exogenous oxytocin, this treatment did restore many of these functions to normal (Grippo, Trahanas, Zimmerman, Porges, & Carter, 2009).
In modern societies, humans can survive, at least after childhood, with little or no human contact. Communication technology, social media, electronic parenting, and many other recent technological advances may reduce social behaviors, placing both children and adults at risk for social isolation and disorders of the autonomic nervous system, including deficits in their capacity for social engagement and love (Porges, 2011).
Social engagement actually helps us to cope with stress. The same hormones and areas of the brain that increase the capacity of the body to survive stress also enable us to better adapt to an ever-changing social and physical environment. Individuals with strong emotional support and relationships are more resilient in the face of stressors than those who feel isolated or lonely. Lesions in various bodily tissues, including the brain, heal more quickly in animals that are living socially versus in isolation (Karelina & DeVries, 2011). The protective effects of positive sociality seem to rely on the same cocktail of hormones that carries a biological message of “love” throughout the body.
Can love—or perhaps oxytocin—be a medicine?
Although research has only begun to examine the physiological effects of these peptides beyond social behavior, there is a wealth of new evidence showing that oxytocin can influence physiological responses to stress and injury. As only one example, the molecules associated with love have restorative properties, including the ability to literally heal a “broken heart.” Oxytocin receptors are expressed in the heart, and precursors for oxytocin appear to be critical for the development of the fetal heart (Danalache, Gutkowska, Slusarz, Berezowska, & Jankowski, 2010). Oxytocin exerts protective and restorative effects in part through its capacity to convert undifferentiated stem cells into cardiomyocytes. Oxytocin can facilitate adult neurogenesis and tissue repair, especially after a stressful experience. We now know that oxytocin has direct anti-inflammatory and antioxidant properties in in vitro models of atherosclerosis (Szeto et al., 2008). The heart seems to rely on oxytocin as part of a normal process of protection and self-healing. Researchers are interested in the medical/therapeutic potential of oxytocin.
Thus, oxytocin exposure early in life not only regulates our ability to love and form social bonds, it also affects our health and well-being. Oxytocin modulates the hypothalamic–pituitary adrenal (HPA) axis, especially in response to disruptions in homeostasis (Carter, 1998), and coordinates demands on the immune system and energy balance. Long-term, secure relationships provide emotional support and down-regulate reactivity of the HPA axis, whereas intense stressors, including birth, trigger activation of the HPA axis and sympathetic nervous system. The ability of oxytocin to regulate these systems probably explains the exceptional capacity of most women to cope with the challenges of childbirth and childrearing.
Dozens of ongoing clinical trials are currently attempting to examine the therapeutic potential of oxytocin in disorders ranging from autism to heart disease. Of course, as in hormonal studies in voles, the effects are likely to depend on the history of the individual and the context, and to be dose-dependent. As this research is emerging, a variety of individual differences and apparent discrepancies in the effects of exogenous oxytocin are being reported. Most of these studies do not include any information on the endogenous hormones, or on the oxytocin or vasopressin receptors, which are likely to affect the outcome of such treatments.
Research in this field is new and there is much left to understand. However, it is already clear that both love and oxytocin are powerful. Of course, with power comes responsibility. Although research into mechanisms through which love—or hormones such as oxytocin—may protect us against stress and disease is in its infancy, this knowledge will ultimately increase our understanding of the way that our emotions impact upon health and disease. The same molecules that allow us to give and receive love also link our need for others with health and well-being.
Conclusion
In this section, we’ve discussed historical and emerging approaches to sexual response. An important take-away to this section is that sexual responsiveness isn’t simply physiological: Psychological factors are also present. At the same time, biology matters and consideration for hormonal and neurological information can be important in our sexual experiences. Keeping an intersectional lens can be a helpful way of learning, evaluating and growing in your own sexual responses.
Licenses and Attributions
Carter, S. & Porges, S. (2021). Biochemistry of love. In R. Biswas-Diener & E. Diener (Eds), Noba textbook series: Psychology. Champaign, IL: DEF publishers. Retrieved from http://noba.to/3629qu8v. Licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License. Permissions beyond the scope of this license may be available in our Licensing Agreement.
Lucas, D. & Fox, J. (2021). Human sexual anatomy and physiology. In R. Biswas-Diener & E. Diener (Eds), Noba textbook series: Psychology. Champaign, IL: DEF publishers. Retrieved from http://noba.to/m28zt7ds. Licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License. Permissions beyond the scope of this license may be available in our Licensing Agreement.
Adaptations: Reformatted. Modified content for language, application to subject and cohesion.
TED’s videos may be used for non-commercial purposes under a Creative Commons License, Attribution–Non Commercial–No Derivatives (or the CC BY – NC – ND 4.0 International)
TEDx Talks. (2016). Confidence and joy are the keys to a great sex life | Emily Nagoski | TEDxUniversityofNevada. https://www.youtube.com/watch?v=HILY0wWBlBM
References
Barmak, S. (2018).The misunderstood science of sexual desire. The Science of Us: The Cut. Retrieved from https://www.thecut.com/2018/04/the-misunderstood-science-of-sexual-desire.html
Carter, S. & Porges, S. (2021). Biochemistry of love. In R. Biswas-Diener & E. Diener (Eds), Noba textbook series: Psychology. Champaign, IL: DEF publishers. Retrieved from http://noba.to/3629qu8v
Hyde, J. S., & DeLamater, J. D. (2017). Understanding human sexuality. McGraw-Hill.
Leiblum, S. R. (2000). CME: Redefining female sexual response. Contemporary Ob/Gyn, 11, 120-134. Retrieved from https://www.contemporaryobgyn.net/view/cme-redefining-female-sexual-response
Lucas, D. & Fox, J. (2021). Human sexual anatomy and physiology. In R. Biswas-Diener & E. Diener (Eds), Noba textbook series: Psychology. Champaign, IL: DEF publishers. Retrieved from http://noba.to/m28zt7ds
Savic, I. (2014). Pheromone processing in relation to sex and sexual orientation. In C. Mucignat-Caretta (Ed), Neurobiology of chemical communication. Boca Raton, FL: CRC Press/Taylor & Francis. https://www.ncbi.nlm.nih.gov/books/NBK200984/
License
Introduction to Human Sexuality by Ericka Goerling & Emerson Wolfe is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License.
