“Let food be thy medicine, and medicine be thy food.”
-Hippocrates, referred to as the “Father of Modern Medicine”
Life depends on nourishment and the quality of life depends greatly on the foods you choose to eat. Any discussion of nutrition must begin with an understanding of nutrition, nutrients, and their overall relationship to health and well-being.
Learning Objectives
- Define health, nutrition, and disease.
- List and describe the characteristics used to assess health status of an individual.
- Explain the difference between primary and secondary nutrient deficiency.
- Differentiate among risk factors, signs, and symptoms.
- Define the word “nutrient” and differentiate among the six classes of nutrients essential for health.
- Explain how energy values of food are determined, and list the three energy-yielding nutrients and their energy contribution.
- Describe measures of food quality and be able to calculate and compare energy densities of foods.
- Describe the importance of research and scientific methods to understanding nutrition.
- Analyze sources of nutrition information for reliability and credibility.
1.1 Defining Nutrition, Health, and Disease
The word nutrition first appeared in 1551 and comes from the Latin word nutrire, meaning “to nourish.” Today, we define nutrition as the sum of all processes involved in how organisms obtain nutrients, metabolize them, and use them to support all of life’s processes. Nutritional science is the investigation of how an organism is nourished, and incorporates the study of how nourishment affects personal health, population health, and planetary health. Nutritional science covers a wide spectrum of disciplines. As a result, nutritional scientists can specialize in particular aspects of nutrition such as biology, physiology, immunology, biochemistry, education, psychology, sustainability, and sociology.
Without adequate nutrition the human body does not function optimally, and severe nutritional inadequacy can lead to disease and even death. The typical American diet contains adequate calories, but is lacking in many ways, from not containing the proper amounts of essential nutrients, to being too speedily consumed, to being only meagerly satisfying.
Registered Dietitians (RD), also called Registered Dietitian Nutritionists (RDN), are nutrition professionals who integrate their knowledge of nutritional science into helping people achieve a healthy diet and develop good dietary habits. Through their knowledge and experiences, RDs/RDNs specialize in translating nutrition science into practical advice. Becoming an RD/RDN requires a college degree with an emphasis in chemistry, anatomy and physiology, and other sciences, the completion of a 1200-hour dietetic internship in clinical and community settings, and passing the national certification exam. Once you achieve RD/RDN status, you must complete 75-hours of continuing education in nutrition every five years. RDs/RDNs work in many diverse settings including hospitals, clinics, long-term care facilities, schools, health clubs, grocery stores, private practice, insurance companies, and corporate wellness programs. They can help you overcome disordered eating, set realistic weight loss and weight management goals, manage chronic diseases, or help you achieve optimal athletic performance. The Academy of Nutrition and Dietetics (AND) is the largest organization of nutrition professionals in the world and dietitians registered with the AND are committed to helping Americans eat well and live healthier lives. To learn more about the AND and their nutritional advice for consumers, visit eatright.org.
Nutrition and Health and Disease
Your ability to wake up, to think clearly, to communicate, to hope, to dream, to go to school, to gain knowledge, to go to work, to earn a living, and to do all of the things that you like to do are dependent upon one factor—your health. Good health means you are able to function normally and work hard to achieve your goals in life. In 1946, the World Health Organization (WHO) defined health as “a state of complete physical, mental, and social well-being, and not merely the absence of disease or infirmity.”1 This definition was adopted into the WHO constitution in 1948 and remains to this day. A triangle is often used to depict the equal influences of physical, mental, and social well-being on health.
Disease is defined as any abnormal condition affecting the health of organisms and typically characterized by specific signs and symptoms. Diseases are broadly categorized as resulting from pathogens (i.e., bacteria, viruses, fungi, and parasites), deficiencies, genetics, and/or physiological dysfunction. Diseases that primarily affect physical health are those that impair body structure (as is the case with osteoporosis), or functioning (as is the case with cardiovascular disease). Mental illnesses primarily affect mental and social well-being.
The foods we eat affect multiple aspects of our health. For example, a teen with type 2 diabetes (a disease often brought on by poor diet and lack of physical activity) is first diagnosed by physical signs and symptoms such as increased urination, excessive thirstiness, and unexplained weight loss. But research has also found that teens with uncontrolled type 2 diabetes often have impaired thinking and may not interact well with others in school, thereby affecting mental and social well-being. This is just one example of a physiological disease that can affect physical, mental, and social aspects of health.
In the early twentieth century, most nutrition-related diseases and conditions were related to inadequate calorie consumption or deficiency of nutrients. In the latter part of the twentieth century nutrition scientists, public health organizations, and the American public increasingly recognized that eating too much of certain foods is linked to chronic diseases. Table 1.1.1 shows the top ten causes of death in the US. As you can see, many of these causes are related to nutrition. We now know that diet-related conditions and diseases include but are not limited to cardiovascular (heart) diseases including hypertension (high blood pressure) and stroke, obesity, type 2 diabetes, several forms of cancer, and osteoporosis.
Table 1.1.1 United States Leading Causes of Death 2017 & 2018 in deaths per 100,000 US Standard Population2
| Cause of Death | 2017 | 2018 |
| All Causes | 731.9 | 723.6 |
| Heart Disease* | 165.0 | 163.6 |
| Cancer* | 152.5 | 149.1 |
| Unintentional Injuries | 49.4 | 48.0 |
| Chronic Lower Respiratory Diseases | 40.9 | 39.7 |
| Stroke* | 37.6 | 37.1 |
| Alzheimer Disease** | 31.0 | 30.5 |
| Diabetes* | 21.5 | 21.4 |
| Influenza and Pneumonia | 14.3 | 14.9 |
| Kidney Disease* | 13.0 | 12.9 |
| Suicide | 14.0 | 14.2 |
| *indicates known relationship to nutrition;
** indicates suspected relationship to nutrition |
||
1.2 Assessing Your Health
There are many factors that determine whether you are “healthy.” Although the WHO definition describes health as not just the absence of disease, but also encompassing psychological, emotional, and social well-being, most of Western medicine is focused on a person’s physical health. As we have discussed previously, and will continue to discuss throughout this course, nutrition plays an enormous role in determining our overall health. Assessing one’s nutritional status can help us determine whether nutritional intake (or lack of) is affecting the development or continuance of nutrition-related health conditions. No one eats 100% healthy foods 100% of the time, but with assessment we look at the overall eating pattern and how it affects overall health. Nutrition assessment uses many tools to help determine whether a person is well-nourished or malnourished (referring to either undernourished or overnourished).
There are six areas to consider when assessing health through a nutrition lens. An easy way to remember these areas is using the letters ABCDEF:
A: anthropometric
B: biochemical
C: clinical
D: dietary
E: environmental
F: family history
A: Anthropometric Assessment
The word anthropometric comes from two terms: anthropo meaning “human” and metric meaning “measure.” There are many different measures used to assess growth in humans including height, weight, body mass index (BMI), head circumference, girth measurements of limbs, waist, hip, and body composition measures such as skinfold/fat fold thickness or bioelectrical impedance analysis. We then compare those measures to known health standards. Often these types of measurements are used to assess the growth of children and adolescents. Some of these measures such as height and weight are used throughout our lifetimes, comparing measurements over time, or comparing one person to another. We will discuss these measures in more detail in Chapter 9 Energy Balance, Chapter 12 Nutrition and Fitness, and Chapter 18 Nutrition Through the Lifecycle.
B: Biochemical Assessment
Biochemical assessment includes laboratory tests that can measure a nutrient or its metabolites in the blood, urine, feces, or other bodily secretions. We can learn quite a bit about a person’s health by looking at these tests and they are routinely collected and examined as part of a general physical by your doctor. In nutrition, for example, we look at the levels of glucose in the blood and in the urine to determine if a person has or is at risk for diabetes. We look at blood cholesterol profiles to help determine risk for some forms of cardiovascular disease. The amount of iron in the blood can indicate a person’s risk for anemia. It is recommended that patients keep copies of routine lab tests to examine trends over time.
C: Clinical Assessment
In addition to anthropometric and biochemical measures, clinical signs and symptoms are used to assess nutritional status such as a potential nutrient deficiency or toxicity. Signs are those things that can be easily seen such as bleeding, vomiting, or fainting. Symptoms are those things that a patient may be experiencing that cannot easily be seen and must be described such as a headache, nausea, dizziness, or pain. Special attention is given to a person’s organs such as skin, eyes, tongue, ears, mouth, hair, nails, and gums. Clinical methods of assessing nutritional status involve checking signs at specific points on the body, or asking patients about any symptoms that may indicate a nutrient deficiency. Often other clinical measures such as temperature and blood pressure are also taken.
If a nutrient deficiency is suspected based on signs or symptoms, often a biochemical test is completed to help identify the exact nutrient that may be inadequate or missing. There are two types of nutrient deficiencies a person may develop. A primary nutrient deficiency occurs when a person does not consume enough of an essential nutrient. A secondary nutrient deficiency occurs when enough of the nutrient is consumed, but for some reason the body is unable to use that nutrient effectively. Secondary nutrient deficiencies can occur because of functional problems in the digestive tract, medications that may be interfering with the body’s absorption or metabolism of a particular nutrient, the body’s natural aging process, and many other reasons.
Primary or Secondary Nutrient Deficiency?
25-year old new mother Carina is complaining of fatigue, some dizziness, and excessive shortness of breath with light exercise. During her pregnancy she was very careful with her diet, and consumed iron supplements during her last trimester. During delivery of her baby, she lost quite a bit of blood. Lab tests currently indicate that her iron levels are extremely low and she has iron deficiency anemia. Do you think Carina has a primary or secondary deficiency of iron?
Answer: Carina would most likely have a secondary deficiency due to blood loss during delivery. However, we could not be 100% sure of this without doing a dietary assessment (see below).
D: Dietary Assessment
Dietary methods of assessment include looking at past and current intake of nutrients from food by individuals or a group to help determine their nutritional status. Completing a dietary assessment is crucial when trying to determine whether or not your intake is related to a disease or condition. There are several methods that may be used to do this:
- 24-hour dietary recall. A trained professional asks a person to recall all food or drink consumed in the previous 24-hours. This is a quick and easy method. However, it is dependent upon the person’s short-term memory and may not be very accurate. It also looks at just one day, which may not be a “typical” day of intake for the individual.
- Food Frequency Questionnaire. The person is given a list of foods and asked to indicate average intake per day, per week, and per month. This method is inexpensive and easy to administer, however it often lacks detail and may not be very accurate. It can still provide a broad overview of one’s overall eating pattern.
- Food Diary. Food intake is recorded at the time of eating. This is also known as a food journal or food record. These diaries can be done with paper and pencil, but are more likely to be recorded using apps on a phone or other electronic device. This method is generally reliable but is difficult to accurately maintain for more than a few days, and portion sizes can be difficult to estimate.
- Observed Food Consumption. This method requires food to be weighed and the nutrient content exactly calculated. It is very accurate, but time consuming and expensive, and is usually done only for research purposes.
E: Environmental Assessment (Lifestyle)
Where and how you live can have a profound effect on your health and nutritional status. Many environmental factors play a role including your living situation (alone, with a family, with friends, etc.), geographic location (urban vs rural, north vs south, etc.), socioeconomic position, access to healthy foods, your ability to prepare food, and other lifestyle factors such as exercise and sleep patterns, emotional health, and work-life balance.
An assessment of your environment includes evaluating not only your nutrition, but also your personal habits. Many diseases are preventable by simply staying away from certain behaviors (smoking, excessive alcohol use, risky sexual activity, etc.). Instead adopt healthful measures like participating in regular physical activity, wearing seat belts in the car and helmets while cycling, and finding healthy ways to minimize your response to stressors like meditation or spending time outdoors. As stated earlier, health is more than just physical. Emotional health is often hard to talk about; however, a person’s quality of life is highly affected by emotional stability. Finding balance between work and life is a difficult and continuous process involving keeping track of your time, taking advantage of job flexibility options, saying no, and finding support when you need it. Work-life balance can influence what you eat too.
F: Family Medical History
Everyone starts out in life with the genes handed down to them from their mother and father. Genes are responsible for your many traits as an individual and are defined as the sequences of DNA that code for all the proteins in your body. The expression of different genes can determine the color of your hair, skin, and eyes, and even if you are more likely to be fat or thin and if you have an increased risk for a certain disease. The sequence of DNA that makes up your genes and determines your genetic makeup is called your genome. In 2003, the Human Genome Project was completed and now the entire sequence of DNA in humans is known. It consists of about three billion individual units and contains between 25,000 and 30,000 genes. The human genome that was sequenced was taken from a small population of donors and is used as a reference DNA sequence for the entire population. Each of us has a similar but unique DNA sequence. Only identical twins and cloned animals have the exact same DNA sequence.
Epigenetics is the study of how your behaviors and your environment may turn genes “on” or “off,” causing changes that can affect how your genes work. In recent years scientists have been studying the possible epigenetic links between genes and nutrients. Initial studies looked at nutrigenomics, the study of the intake of nutrients and their effects on genetic expression in an individual. Not all epigenetic changes are permanent. A beneficial change in nutrient intake, increased physical activity, or quitting smoking can reverse some epigenetic modifications and improve health.
A second way to look at the interplay between nutrients and genes is to identify genetic markers in individuals that may modify their need for or use of various nutrients which may influence health outcomes. This is called nutrigenetics. Genetic differences may help explain why some people achieve weight loss with certain diets and others do not. Or whether a person may benefit more from a low sodium diet than someone else might. You may see internet sites touting personalized nutrition, their ability to help you (for a hefty fee), “eat right for your genes.” Although this is an exciting area of research, the science is complicated. Be sure that if you access these services, that there is a health professional such as an RD/RDN who can help you interpret your individual results.
Because genetics play a large role in defining your health it is a good idea to learn whether there are some diseases and conditions that may be more likely to affect you based on your inherited genes. To do this, record your family’s medical history. Start by drawing a chart that lists your immediate family and relatives. The next time you attend a family event or see extended family members, start filling in the blanks. What did people die from? What country did Grandpa come from? While this may be an interesting project historically, it can also provide you with a practical tool to determine to what diseases you might be more susceptible. This will allow you to make better dietary and lifestyle changes early on to help prevent a disease from being handed down from your family to you. It is good to compile your information from multiple relatives.
Risk Factors
Assessing your current health status based on these six categories can help you identify some of your risk factors. A risk factor is something that makes you more likely to develop adverse health conditions. Some risk factors are inherited through your genes as discussed previously. These risk factors are part of your DNA, but may be affected by your health behaviors, either positively or negatively. However, scientists consider them non-modifiable because they are part of your genetic code which cannot be altered. Other risk factors such as biological sex, age, and race are also non-modifiable. Some risk factors are modifiable because they are choices an individual makes each day. For example, if you smoke you are more likely to develop lung cancer than someone who does not smoke. Thus smoking is a risk factor for lung cancer. Some people can smoke for years and never develop lung cancer, while others may develop lung cancer and never smoke. However, the chances that you will develop lung cancer if you’re a smoker are much higher than if you never smoked. If you quit smoking, you may reduce your risk of developing this terrible disease. Obesity, physical inactivity, and dietary factors such as low fiber intake and high saturated fat intake are risk factors for many different health conditions including heart disease, type 2 diabetes, and some forms of cancer. Choosing healthier meals and exercising regularly can go a long way to reducing the chances that you will develop one of these debilitating health conditions. The more risk factors you have for a health condition the more likely you are to eventually suffer from it. Assessing your health using ABCDEF allows you to identify your current risk factors and to take steps to modify those you can.
Risk Factors vs Signs or Symptoms
Many people confuse risk factors with signs or symptoms of disease, but they are different. Risk factors occur prior to development of a disease. They make you more likely to develop the disease, but not everyone with a risk factor will. You will experience signs and symptoms when you have a condition. Common signs and symptoms of type 2 diabetes, for example, include frequent urination, excessive thirst, frequent hunger, tingling in the extremities, and others. These occur during and after the development of the disease. To reiterate, risk factors occur prior to disease development. The more risk factors you have for a health condition (both modifiable and non-modifiable) the more likely you are to develop that condition. Signs and symptoms are experienced once you develop the condition.
1.3 Nutrients
As we saw in the previous section, many different factors affect our overall health and well-being. In this course our primary focus is on the role of dietary nutrient intake and nutrient functions in body processes.
Our bodies require dozens of different chemicals found in food to help us maintain optimal health. These chemicals are called nutrients , and the study of how these chemicals interact with each other and with our bodies is called nutrition. Nutrients are substances required by the body to perform its basic functions. We consume our favorite foods and beverages (and sometimes our not so favorites) in an attempt to gain all of the necessary nutrients to achieve or maintain our health. Sometimes we also consume supplements in addition to foods to be sure we are getting all of the required nutrients.
Although all nutrients are important, scientists categorize some as essential. The word essential means we have to have it, however, in nutrition the word essential also means we have to obtain it from an outside source, from foods or beverages. In other words, an essential nutrient is one we need that we have to consume. Non-essential nutrients are also necessary and vital for good health, but these nutrients can be made by the body in sufficient amounts as long as adequate essential nutrients are consumed, and don’t necessarily need to be a part of our daily dietary intake. Sometimes a formerly non-essential nutrient may become conditionally essential. This means that under normal circumstances a person could manufacture what they need, but if, for example, they are taking a certain medication or have a medical condition that modifies their ability to make the nutrient, then they must consume it.
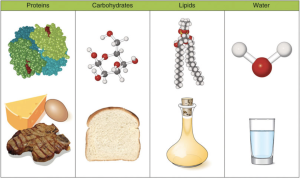
Nutrients are used to help us produce energy, detect and respond to environmental surroundings, move, excrete wastes, respire (breathe), grow, and reproduce. To make it easier to study nutrients, we combine those that have similar properties or functions into groups or “classes.” There are six classes of nutrients required for the body to function and maintain overall health. These classes are carbohydrates, protein, lipids, water, vitamins, and minerals.
Table 1.3.1 Classes of Nutrients and their Basic Functions
| Nutrient Class | Basic Functions |
| Carbohydrates | Provide a ready source of energy for the body and provide structural constituents for the formation of cells. |
| Protein | Necessary for tissue formation, cell repair, production of hormones/enzymes/neurotransmitters. Essential for building muscle and a healthy immune system. |
| Lipids | Provide stored energy for the body, functions as structural components of cells, and also as signaling molecules for proper cellular communication. Provides insulation to vital organs and works to maintain body temperature. |
| Vitamins | Regulate body processes and promote normal body system functions. |
| Minerals | Regulate body processes, necessary for proper cellular function, and comprise body tissue. |
| Water | Transports essential nutrients to all body parts, transports waste products for disposal, and aids with body temperature maintenance. |
Macronutrients
Nutrients that are needed in large amounts are called macronutrients. There are four classes of macronutrients: carbohydrates, protein, lipids, and water. Of these macronutrients, three (carbohydrate, protein, and lipids) can be metabolically processed into cellular energy and thus are called energy nutrients. The energy from macronutrients comes from their chemical bonds. This chemical energy is converted into cellular energy in the form of adenosine triphosphate (ATP) that is then utilized to perform work, allowing our bodies to conduct their basic functions. Water is also a macronutrient in the sense that you require a large amount of it, but unlike the other macronutrients it does not yield calories.
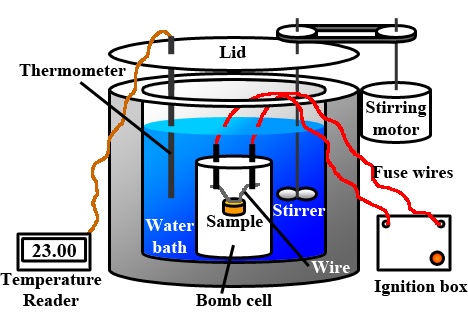
A unit of measurement of food energy is the calorie (denoted with a small “c”). A calorie is the amount of energy required to raise 1 gram of water 1° Celsius. On nutrition food labels and in the field of nutrition the amount given for “Calories” is actually equivalent to each calorie multiplied by one thousand. A kilocalorie or kcal (one thousand calories, denoted with a small “c”) is synonymous with the “Calorie” (denoted with a capital “C”). When you see Calories on nutrition food labels it is equal to kcals (Calorie = kcal). Therefore, you can use “kcal” to denote amounts of energy from food (as we have done throughout this text).
Carbohydrates
Carbohydrates are molecules composed of carbon, hydrogen, and oxygen. Any molecule that contains carbon atoms is considered an organic molecule. This use of the term organic refers only to the molecule’s chemical composition and is different from the use of the term organic in relation to how foods are grown. The main function of carbohydrates is to provide energy. The major food sources of carbohydrates are grains, milk, fruits, and starchy vegetables like potatoes. Non-starchy vegetables like broccoli or kale also contain carbohydrates, but in lesser quantities. Carbohydrates are almost exclusively found in plant-based foods. Carbohydrates are broadly classified into two forms based on their chemical structure: simple and complex.
One gram (g) of carbohydrates yields 4 kcal of energy for the cells in the body to perform work. In addition to providing energy and serving as building blocks for bigger macromolecules, carbohydrates are essential for proper functioning of the nervous system, heart, and kidneys.
All carbohydrates are made up of building blocks called monosaccharides, the most common monosaccharide is glucose. Some carbohydrates such as table sugar or honey are made of just two monosaccharides, so are called simple carbohydrates. Other carbohydrates are made up of hundreds or thousands of monosaccharides, and are called complex. Glucose can be stored for future use. In animals including humans, the storage molecule of carbohydrates is called glycogen and in plants it is known as starch. Glycogen and starches are complex carbohydrates, as is dietary fiber.
Proteins
Proteins are organic molecules composed of chains of amino acids. Amino acids are simple sub-units composed of carbon, oxygen, hydrogen, and nitrogen. The food sources of proteins are meats, dairy products, seafood, and a variety of different plant-based foods, most notably soy. The word protein comes from a Greek word meaning “of primary importance,” which is an apt description of these macronutrients; they are also known colloquially as the “workhorses” of life. Proteins provide 4 kcal of energy per g; however providing energy is not protein’s most important function. Proteins provide structure to bones, muscles and skin, they make up hormones, enzymes, neurotransmitters, and molecules important in immunity, and play a role in conducting most of the chemical reactions that take place in the body. Scientists estimate that greater than 20,000 different proteins exist within the human body.
Lipids
Lipids are also a family of organic molecules composed of carbon, hydrogen, and oxygen, but unlike carbohydrates, they are insoluble in water. Lipids are found predominantly in butter, oils, meats, dairy products, nuts, and seeds, and in many processed foods. The three main types of lipids are triglycerides (or triacylglycerols), phospholipids, and sterols. The main job of lipids is to store energy. Lipids provide more energy per g than carbohydrates or protein (9 kcal per g of lipids versus 4 kcal per g of carbohydrates/protein). In addition to energy storage, lipids serve as components of cell membranes, surround and protect organs, aid in temperature regulation, and regulate many other functions in the body.
Water
There is one other nutrient that we must consume in large quantities: water. Water does not contain carbon, making it an inorganic molecule. It is composed of two hydrogen (H2) and one oxygen (O) per one molecule of water. More than 60% of your total body weight is water. Without it, nothing could be transported in or out of the body, chemical reactions would not occur, organs would not be cushioned, and body temperature would fluctuate widely. On average, an adult consumes just over two liters of water per day from food and drink. According to the “rule of threes,” a generalization supported by survival experts, a person can survive three minutes without oxygen, three days without water, and three weeks without food. Since water is so critical for life’s basic processes, the amount of water input and output is supremely important. However, water does not provide any kcal. So it is considered a macronutrient, but not an energy nutrient.
Alcohol
Alcohol is not considered a nutrient, although it is a source of kcal. Remember that a nutrient is something that is necessary for body functioning and overall health. Alcohol does not meet that definition of a nutrient. Alcohol itself provides approximately 7 kcal for every g consumed. In addition to alcohol, many alcoholic drinks contain additional kcal from other nutrient classes—especially carbohydrates.
Micronutrients
Micronutrients are nutrients required by the body in very small amounts, but are still essential for carrying out bodily functions. Micronutrients include all the essential minerals and vitamins. There are 13 essential vitamins and 16 minerals (see Table 1.3.2 and Table 1.3.3 for a complete list and their major functions). In contrast to carbohydrates, protein, and lipids, micronutrients are not directly used for making energy and do not contain kcal, but they assist in the process of energy production as part of enzymes (i.e., coenzymes). Enzymes are proteins that catalyze chemical reactions in the body and are involved in all aspects of body functions from producing energy, to digesting nutrients, to building macromolecules. Micronutrients play many roles in the body.
Vitamins
The 13 vitamins are categorized as either water-soluble or fat-soluble. The water-soluble vitamins are vitamin C and all the B vitamins, which include thiamin, riboflavin, niacin, pantothenic acid, B6, biotin, folate and B12. The fat-soluble vitamins are A, D, E, and K. Vitamins are required to perform many functions in the body such as making red blood cells, synthesizing bone tissue, and playing a role in normal vision, nervous system function, and immune system function.
Vitamin deficiencies can cause severe health problems. For example, a deficiency in niacin causes a disease called pellagra, which was common in the early twentieth century in some parts of America. The common signs and symptoms of pellagra are known as the “4D’s—diarrhea, dermatitis, dementia, and death.” Until scientists found out that better diets relieved the signs and symptoms of pellagra, many people with the disease ended up in asylums awaiting death. The deficiency of other vitamins was found to cause other disorders and diseases such as scurvy (vitamin C), night blindness (vitamin A), and rickets (vitamin D).
Table 1.3.2 Vitamins and Their Major Functions
| Vitamins | Major Functions |
| Water-soluble | |
| Thiamin (B1) | Coenzyme, energy metabolism assistance |
| Riboflavin (B2) | Coenzyme, energy metabolism assistance |
| Niacin (B3) | Coenzyme, energy metabolism assistance |
| Pantothenic acid (B5) | Coenzyme, energy metabolism assistance |
| B6 (Pyroxidine) | Coenzyme, amino acid synthesis assistance |
| Biotin (B7) | Coenzyme |
| Folate (B9) | Coenzyme, essential for growth |
| B12 (Cobalamin) | Coenzyme, red blood cell synthesis |
| C | Collagen synthesis, antioxidant |
| Fat-soluble | |
| A | Vision, reproduction, immune system function, antioxidant |
| D | Bone and teeth health maintenance, immune system function |
| E | Antioxidant, cell membrane protection |
| K | Blood clotting, bone and teeth health maintenance |
Minerals
Minerals are solid inorganic substances that form crystals and are classified depending on how much of them we need. Trace (minor) minerals such as molybdenum, selenium, zinc, iron, and iodine, are only required in a few milligrams (mg) or less per day while major minerals such as calcium, magnesium, potassium, sodium, and phosphorus, are required in hundreds of mg. Like vitamins, minerals do not contain kcal. Many minerals are critical for enzyme function, others are used to maintain fluid balance, build bone tissue, synthesize hormones, transmit nerve impulses, contract and relax muscles, and protect against harmful free radicals.
Table 1.3.3 Minerals and Their Major Functions
| Minerals | Major Functions |
| Major | |
| Sodium | Fluid balance, nerve transmission, muscle contraction |
| Chloride | Fluid balance, stomach acid production |
| Potassium | Fluid balance, nerve transmission, muscle contraction |
| Calcium | Bone and teeth health maintenance, nerve transmission, muscle contraction, blood clotting |
| Phosphorus | Bone and teeth health maintenance, acid-base balance |
| Magnesium | Protein production, nerve transmission, muscle contraction |
| Sulfur | Protein production |
| Trace/Minor | |
| Iron | Carries oxygen, assists in energy production |
| Zinc | Protein and DNA production, wound healing, growth, immune system function |
| Iodine | Thyroid hormone production, growth, metabolism |
| Copper | Coenzyme, iron metabolism |
| Selenium | Antioxidant |
| Chromium | Assists insulin in glucose metabolism |
| Manganese | Coenzyme |
| Molybdenum | Coenzyme |
| Fluoride | Bone and teeth health maintenance, tooth decay prevention |
To review, the dozens of nutrients that the body requires are grouped into six classes based on form and function. Below is a summary of the characteristics of the six nutrient classes.
Table 1.3.4 Summary of Nutrient Class Characteristics
| Class of Nutrient | Macro- or Micronutrient | Organic Nutrient (contains carbon) | Energy Nutrients |
| Carbohydrates | Macro | Yes | Yes – 4 kcal/g |
| Protein | Macro | Yes | Yes – 4 kcal/g |
| Lipids | Macro | Yes | Yes – 9 kcal/g |
| Vitamins | Micro | Yes | No |
| Minerals | Micro | No | No |
| Water | Macro | No | No |
Food Energy
As discussed previously, food energy is measured in Calories and commonly referred to as kcal. Though this is only the first chapter, you have already seen the words “kcal” and “energy” used several times. In everyday life you have probably heard people talk about how many kcal they burned on the treadmill or how many calories are listed on a bag of chips. Kcal are a measure of energy. It takes quite a lot of kcal to keep us alive. Even if a person is in a coma, they still burn approximately 1000 kcal of energy in order for their heart to beat, their blood to circulate, their lungs to breathe, etc. We burn even more kcal when we exercise. A food’s kcal are determined by putting the food into a bomb calorimeter, heating it, and determining the energy output (energy = heat produced). The carbohydrates, proteins, and fats we eat and drink provide kcal for us (and alcohol as well if we choose to consume it).
Food Quality

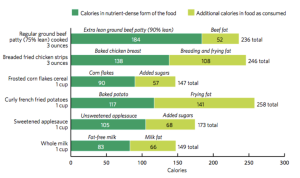
One measurement of food quality is the amount of nutrients it contains relative to the amount of energy it provides. High quality foods are nutrient dense, meaning they contain many nutrients relative to the amount of calories they provide. A food with high nutrient density would have a large amount of various beneficial nutrients in each “bite” of that particular food. Because “bites” are different for everyone, we use common measures such as gram (g), ounce (oz), cup (c), pound (lb), liter (L), tablespoon (tbs), etc. to help us compare different foods. (See common measures used in Appendix 1). Determining nutrient density of a food is not straightforward. One must consider the nutrient profile of a food as a whole, and it can be quite subjective. However, it is generally agreed that whole fruits and vegetables, 100% whole grains, nuts, and legumes tend to have high nutrient density. Food quality is additionally associated with its taste, texture, appearance, microbial content, and how much consumers like it.
Another measure of food quality is to examine the number of kcals in a food relative to the size of each “bite.” The term used to describe this is energy density or calorie density. Foods high in fats and sugars, like fast food burgers, pizza, candy bars, etc. would be considered energy dense since they provide many calories per bite but are typically lacking several essential vitamins, minerals, and other beneficial nutrients like fiber. We can compare the energy density of different foods if we know the number of kcals and the size of a serving for each.
A third term often used to describe food quality is “empty calorie.” Foods such as carbonated sugary soft drinks provide many calories, but very few, if any, beneficial nutrients, making the calories “empty.”
We can compare meals to examine food quality:
Let’s say we have a choice between two different breakfasts depicted in Figures 1.3.5 and 1.3.6. Each breakfast contains 500 kcal. But breakfast #2 provides many more nutrients in those 500 kcal than do the donuts. There are several different vitamins and minerals in the two types of berries and in the spinach. These fruits and vegetable also contain fiber, and there is lean protein in the eggs.

The donuts in breakfast #1 contain 500 kcal as well, but those kcals are primarily fat and sugar. There are very few vitamins or minerals in the donuts, and almost no fiber or protein. Therefore, breakfast #2 is more nutrient dense.
We can also compare the energy density of the two breakfasts. Because we know the weights of the two (in grams) and that both contain 500 kcal, we can calculate the energy density of each breakfast.

Energy density of breakfast #1: 500 kcal/135 g = 3.7 kcal per gram of food
Energy density of breakfast #2: 500 kcal/350 g = 1.4 kcal per gram of food
Breakfast #1 has more than 2.5 times as many kcal per gram of food than breakfast #2. Therefore breakfast #1 has higher energy density.
Super Foods
Often you see lists of “Super Foods” on the internet or in magazines. These superfoods (also called “functional foods”) are generally understood to be a food, or a food ingredient, that may provide a health benefit beyond the traditional nutrients it contains.3 These functional foods tend to be whole (not processed) vegetables and fruits like kale or Swiss chard, legumes, or berries, or animal foods like cold water fish. They are considered highly nutritious because they contain not only beneficial nutrients, but also additional beneficial chemical compound(s) that are not nutrients (also called non-nutritive).
Phytochemicals are non-nutritive chemical compounds found in plants (phyto) that provide characteristics to the plant like color, taste, smell. They are found in the edible parts of plants, especially the skin or peel. However, these plant chemicals are also believed to provide health benefits beyond the traditional nutrients. According to the Harvard Medical School, it is estimated that about 5,000 have been identified so far, but we don’t yet know what they all do.4 General categories of phytochemicals include (but are not limited to) carotenoids, flavonoids, and phenols.
Diets rich in fruits and vegetables have been associated with decreased risk of chronic diseases. Many fruits and vegetables are rich in phytochemicals, especially when consumed whole, leading some to hypothesize that phytochemicals are responsible for the decreased risk of chronic diseases. The role that phytochemicals play in health is still in the early stages of research. But you may be able to reduce your risk of chronic disease by consuming high amounts of whole fruits and vegetables to raise your intake of these phytochemicals. However, benefits seem to only come from the plant itself, and not from dietary supplements containing the phytochemical.
1.4 Nutrition Research and the Scientific Method
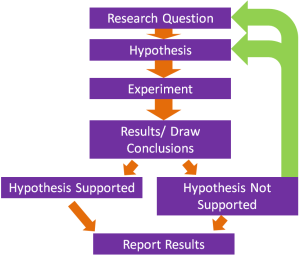
Similar to the method by which a police detective finally charges a criminal with a crime, nutritional scientists discover the health effects of food and its nutrients by first making an observation. Once observations are made, they come up with a hypothesis, test their hypothesis, and then interpret the results. After this, they gather additional evidence from multiple sources and finally come up with a conclusion on whether the food suspect fits the claim. This organized process of inquiry developed in the 17th century is used in the sciences including nutritional science, and is called the scientific method.
One example of how the scientific method has been used in nutritional sciences is in the identification of the mineral iodine and it’s role in the thyroid gland. In the early 1800s the development of an enlargement of the neck, known as a goiter, was common in the population, especially in those living far from the sea. It was thought to be caused by poor hygiene. Because of the use of the scientific method, we now know that a goiter develops when iodine in the diet is deficient. Below is a description of how this was determined.
In 1811, French chemist Bernard Courtois was isolating saltpeter for producing gunpowder to be used by Napoleon’s army. To carry out this isolation he burned some seaweed and, in the process, observed an intense violet vapor that crystallized when he exposed it to a cold surface. He sent the violet crystals to an expert on gases, Joseph Gay-Lussac, who identified the crystal as a new element. It was named iodine, the Greek word for violet. The following scientific record is some of what took place in order to conclude that iodine is a nutrient using the steps of the scientific method: observation, hypothesis, experimental test, interpretation of results.5 Share your results with other scientists. Repeat these steps to gather more evidence until you have enough evidence to reach a conclusion.
Steps of the Scientific Method used to identify Iodine
Observation. Eating seaweed is a cure for goiter, an enlargement of the thyroid gland in the neck.

Hypothesis. In 1813, Swiss physician Jean-Francois Coindet hypothesized that the seaweed contains iodine and he could use just iodine instead of seaweed to treat his patients.
Experimental test. Coindet administered iodine tincture orally to his patients with goiter.
Interpret results. Coindet’s iodine treatment was successful.
Gathering more evidence. Many other physicians contributed to the research on iodine deficiency and goiter.
Hypothesis. French chemist Chatin proposed that the low iodine content in food and water of certain areas far away from the ocean were the primary cause of goiter and renounced the theory that goiter was the result of poor hygiene.
Experimental test. In the late 1860s the program, “The stamping-out of goiter,” started with people in several villages in France being given iodine tablets.
Results. The program was effective and 80% of children with goiter were cured.
Hypothesis. In 1918, Swiss doctor Bayard proposed iodizing salt as a good way to treat areas where much of the population suffered from goiter.
Experimental test. Iodized salt was transported by mules to a small village at the base of the Matterhorn where more than 75% of school children had goiter. It was given to families to use for six months.
Results. The iodized salt was beneficial in treating goiter in this remote population.
Experimental test. Physician David Marine conducted the first experiment of treating goiter with iodized salt in America in Akron, Ohio.6
Results. This study conducted on over 4,000 school children found that iodized salt prevents goiter.
Conclusions. Seven other studies similar to Marine’s were conducted in Italy and Switzerland that also demonstrated the effectiveness of iodized salt in treating goiter. In 1924, US public health officials initiated the program of iodizing salt and started eliminating the scourge of goiterism. Today more than 70% of American households use iodized salt and many other countries have followed the same public health strategy to reduce the health consequences of iodine deficiency.
This is just one example of how the scientific method was used to determine how to treat a specific health condition. There have been millions of studies using this method, and you are benefitting from the results of these studies when you take a medication for a specific disease or condition, or when you modify a behavior to achieve a desired result.
Food for Thought
What are some of the ways in which you think like a scientist and use the scientific method in your everyday life? Any decision-making process uses at least pieces of the scientific method. Think about some of the major decisions you have made in your life and the research you conducted that supported your decision. For example, what computer brand do you own? Where is your money invested? What college do you attend?
Evidence-Based Approach to Nutrition
It took more than 100 years from iodine’s discovery as an effective treatment for goiter until public health programs recognized it as such. Although a lengthy process, the scientific method is a productive way to define essential nutrients and determine their ability to promote health and prevent disease. The scientific method is part of the overall evidence-based approach to designing nutritional guidelines. An evidence-based approach to nutrition includes7:
- Defining the problem or uncertainty (e.g., the rate of colon cancer is higher in people who eat red meat)
- Formulating it as a question (e.g., does eating red meat contribute to colon cancer?)
- Setting criteria for quality evidence
- Evaluating the body of evidence
- Summarizing the body of evidence and making decisions
- Specifying the strength of the supporting evidence required to make decisions
- Disseminating the findings
The Food and Nutrition Board of the National Academy of Medicine (NAM) [formerly known as the Institute of Medicine (IOM)], a non-profit, non-governmental organization, constructs its nutrient recommendations (i.e., Dietary Reference Intakes, or DRI) using an evidence-based approach to nutrition. The entire procedure for setting the DRI is documented and made available to the public. The same approach is used by the US Department of Agriculture (USDA) and US Department of Health and Human Services (HHS). The USDA and HHS websites are great tools for discovering ways to optimize health; however, it is important to gather nutrition information from multiple resources as there are often differences in opinion among various scientists and public health organizations.
Types of Scientific Studies
There are many types of scientific studies that can be used to test a particular hypothesis including epidemiological studies, interventional clinical trials, and randomized clinical interventional trials.
Table 1.4.1 Types of Scientific Studies
| Type | Description | Example | Notes |
| Epidemiological | Observational studies of populations around the world describing the frequency, distribution and patterns of health events over time | Diets with a high consumption of saturated fats are associated with an increased risk of heart attacks | Does not determine cause-and-effect relationships |
| Intervention Clinical Trials | Scientific investigations where a variable is changed between groups | Testing the effect of different diets on blood pressure. Group 1 consumes a typical American diet, group 2 eats a diet rich in fruits and vegetables, and group 3 eats a combination of groups 1 and 2 | If done correctly, it does determine cause-and-effect relationships. But compliance is often difficult |
| Randomized Clinical Trials | Participants are assigned by chance to separate groups that compare different treatments. Neither the researchers nor the participants can choose which group a participant is assigned | Testing the effect of calcium supplements on women with osteoporosis. Participants are given a pill daily of a placebo or calcium supplement. When “double blinded” neither the participants nor the researcher know what group the participant is in | Considered the “gold standard” for scientific studies |
| Animal and Cellular Biology | Studies are conducted on animals or on human cells | Testing the effects of a new blood pressure drug on guinea pigs; or on the lipid membrane of a cell | Less expensive than human trials. However, results may not be applicable, since study not done on the whole person |
Epidemiological studies observe what is actually happening in a population in relation to health over time. The goal is to find factors associated with an increased or decreased risk for a health event, though these sometimes remain elusive. Often these types of studies can help refine a hypothesis. They can be used to predict future health needs, but cannot directly determine if one variable causes another.
Interventional clinical trial studies are scientific investigations in which a variable is changed between groups of people. When well done, this type of study allows one to determine causal relationships. A randomized clinical interventional trial is a study in which participants are assigned by chance to separate groups that compare different treatments. Neither the researchers nor the participants can choose or know which group a participant is assigned to. That’s called a “double blind” study. In these types of studies, the control group usually receives a placebo instead of the actual intervention. These are powerful tools to provide supporting evidence for a particular relationship and are considered the “gold standard” of scientific studies.
The attributes of high quality clinical interventional trial studies are:
- those that include a control group, which does not receive the intervention, to which you can compare the people who receive the intervention being tested.
- those in which the subjects are randomized into groups, meaning a given subject has an equal chance of ending up in either the control group or the intervention group. This is done to ensure that any possible confounding variables are likely to be evenly distributed between the control and the intervention groups.
- “double-blinded” studies in which neither the researchers nor the participants know into which group they have been assigned. This is done to reduce bias on the part of the researchers.
- those studies that include a sufficient number of participants (signified by “n”). Generally the higher the “n” the more robust and significant is the study.
The limitations of clinical intervention studies are that they are difficult to carry on for long periods of time, are costly, and require that participants remain compliant with the intervention. Furthermore, it is unethical to study certain interventions. (An example of an unethical intervention would be to advise one group of pregnant mothers to drink alcohol to determine the effects of alcohol intake on pregnancy outcome, because we know that alcohol consumption during pregnancy damages the developing fetus.)
Because of the types of study limitations it is clear that epidemiological studies complement interventional clinical trial studies and BOTH are necessary to construct strong foundations of scientific evidence for health promotion and disease prevention.
Other scientific studies used to provide supporting evidence for a hypothesis include laboratory studies conducted on animals or cells. An advantage of this type of study is that they typically are less expensive than human studies and they require less time to conduct. Other advantages are that researchers have more control over the environment and the amount of confounding variables can be significantly reduced. Moreover, animal and cell studies provide a way to study relationships at the molecular level and are also helpful in determining the exact mechanism by which a specific nutrient causes a change in health. The main disadvantage of these types of studies is that researchers are not working with whole humans and thus the results may not be as applicable. Nevertheless, well-conducted animal and cell studies that can be repeated by multiple researchers and obtain the same conclusion are definitely helpful in building the evidence to support a scientific hypothesis.
Science is always moving forward, often slowly. One study is not enough to make a guideline or a recommendation or cure a disease. Science is a step-by-step, gradual process that builds on past evidence and finally culminates into a well accepted conclusion. Unfortunately, not all scientific conclusions are developed in the interest of human health and it is important to know where a scientific study was conducted and who provided the funding for the study. This can help you identify bias. Bias means that a researcher or group prefers one outcome over another, so they do not give all possible outcomes an equal chance. If you read an air quality study paid for by a tobacco company that found that smoking did not reduce indoor air quality, you would be skeptical of that result. You should also be skeptical of one on the benefits of red meat performed at a laboratory funded by a national beef association, or the benefits of a dietary supplement paid for by a supplement manufacturing corporation.
Science can also be contentious even among experts that do not have any conflicting financial interests. Contentious science is actually a good thing as it forces researchers to be of high integrity, well-educated, well-trained, and dedicated. It also instigates public health policy makers to seek out multiple sources of evidence in order to support a new policy. Agreement involving many experts across multiple scientific disciplines is necessary for recommending dietary changes to improve health and prevent disease. Although a somewhat slow process, it is better for our health to allow the evidence to accumulate before incorporating some change in our diet.
1.5 Nutrition and the Media
A motivational speaker once said, “A smart person believes half of what they read. An intelligent person knows which half to believe.” In this age of information where instant Internet access is just a click away, it is easy to be misled if you do not know where to go for reliable nutrition information. There are a few websites that can be consistently relied upon for accurate material that is updated regularly.
Using Eyes of Discernment
“New study shows that margarine contributes to arterial plaque.”
“Asian study reveals that two cups of coffee per day can have detrimental effects on the nervous system.”
“Stack your snacks to add three pounds of muscle.”
How do you react when you read news of this nature? Do you boycott margarine and coffee? Change your snacking habits? Nutrition-related hyperbolic headlines and advertisements have been around for decades. In the 1930s there were ads recommending a “reducing soap” that would wash away fat and years of age. In the 1950s and 60s you could reduce your weight by listening to certain music, or by rubbing an “electric spot reducer” over your abdomen. We still see similar types of advertisements on food packaging, and in print and social media. Advertisers use authority figures like actors dressed in white lab coats to convince consumers that a product is healthful. They often use anecdotal evidence (stories) like before and after pictures or warped statistics or single research studies that may contain bias to exaggerate the benefits of a weight loss plan or “health” food. But this type of advertising and these sorts of headlines seem to work. Consumers spend billions of dollars each year on special health foods and beverages or dietary supplements even though the scientific evidence that these substances live up to their hype is sorely lacking.
So what should we as consumers believe? When reading nutrition-related claims, articles, websites, or advertisements always remember that one study does not substantiate a fact. One study neither proves or disproves anything. Readers who may be looking for complex answers to nutritional dilemmas can quickly misconstrue such statements and be led down a path of misinformation. Listed below are ways that you can develop discerning eyes when reading nutritional news.
- The scientific study under discussion should be published in a peer-reviewed journal, such as the Journal of the Academy of Nutrition and Dietetics. Question studies that come from less trustworthy sources (such as non peer-reviewed journals, popular magazines, or websites) or that are not published.
- The report should disclose the methods used by the researcher(s). Did the study last for 3 or 30 weeks? What was the “n” (number of subjects)? The longer the study and the higher the number of subjects, the more robust and credible are the results. What did the participants actually do? Did the researcher(s) observe the results themselves or did they rely on self reports from study participants? Was there a control group who did not receive the treatment so that scientists can compare one group to another?
- Who were the subjects of this study? Humans or animals? If human, are any traits/characteristics noted? Were confounding variables assessed? How were subjects assigned to groups (randomness)? For example, the results of a study of the effects of a dietary supplement on the hearts of cardiac patients should not be used to convince an athlete to take a dietary supplement to improve their own heart’s ability to exercise. These two types of people are quite different. You may realize you have more in common with certain program participants and can use that as a basis to gauge if the study applies to you (age, biological sex, fitness level, underlying medical conditions, geographical location, etc.)
- Credible reports often disseminate new findings in the context of previous research. A single study on its own gives you very limited information, but if a body of literature supports a finding, it gives you more confidence in it.
- Peer-reviewed articles published in well-respected scientific journals deliver a broad perspective and are inclusive of findings of many studies on the exact same subject. By providing a list of previously published articles related to the topic, one can see how a particular study fits into the totality of the research.
- When reading news, ask yourself, “Is this making sense?” Even if coffee does adversely affect the nervous system, do you drink enough of it to see any negative effects? Remember, if a headline professes a new remedy for a nutrition related topic, it may well be a research supported piece of news, but more often than not it is a sensational story designed to catch the attention of an unsuspecting consumer. Track down the original journal article to see if it really supports the conclusions being drawn in the news report.
There are thousands of websites that contain nutrition information. When reading information on websites, Johns Hopkins University recommends that you remember the following criteria for discerning if a site is valid and the information credible8:
Accuracy. Does the website use reliable research? Check many sources for the same information—are the results the same?
Authority. Websites that end in .gov or .edu (and sometimes .org), are usually the most reliable websites for health facts. Make sure the website is written by doctors, dietitians, or other experts in the health field.
Bias. Who pays for the website? If a company supports a website (usually through advertising) they may have control over the website and encourage inaccurate or misleading information that promotes a need for their product or service.
Currency. When were the facts last updated? Medical research never stops. Make sure the information is no older than 3 years.
Some non-profit, non-governmental organizations like Health on the Net (HON), affiliated with the WHO, promote transparency and reliable health information on the internet. For a fee, health-related websites can have their content checked by medical experts from these organizations for accuracy and reliability. If a website becomes certified, it will be allowed to post the organization’s logo on their site for a specified time period (usually 5 years).9 Other organizations like the Utilization Review Accreditation Commission (URAC) have a Health Website accreditation program that looks at both content and security settings for these sites. While these certifications do not guarantee that everything on the website is accurate or reliable, it does provide some level of assurance that the information has some validity.10
Trustworthy Sources
For a list of reliable sources that advocate good nutrition to promote health and prevent disease using evidence-based science see Table 1.5.1. In Chapter 2, we will further discuss nutrition recommendations for Americans.
Table 1.5.1 Web Resources for Nutrition and Health
| Organization | Website |
| Governmental | |
| USDA | http://www.usda.gov/wps/portal/usda/usdahome |
| USDA Center for Nutrition Policy and Promotion | http://www.cnpp.usda.gov/ |
| US Department of Health and Human Services | http://www.hhs.gov/ |
| Centers for Disease Control and Prevention | http://www.cdc.gov/ |
| Food and Drug Administration | http://www.fda.gov/ |
| Healthy People | http://www.healthypeople.gov/2020/default.aspx |
| Office of Disease Prevention and Health Promotion | http://odphp.osophs.dhhs.gov/ |
| International | |
| World Health Organization | http://www.who.int/en/ |
| Food and Agricultural Organization of the United Nations | http://www.fao.org/ |
| Nongovernmental | |
| Harvard School of Public Health | http://www.hsph.harvard.edu/nutritionsource/index.html |
| Mayo Clinic | http://www.mayoclinic.com/ |
| Linus Pauling Institute | http://lpi.oregonstate.edu/ |
| American Society for Nutrition | http://www.nutrition.org/ |
| American Medical Association | http://www.ama-assn.org/ |
| American Diabetes Association | http://www.diabetes.org/ |
| The Academy of Nutrition and Dietetics | http://www.eatright.org/ |
| National Academy of Medicine: Food and Nutrition Board | https://www.nationalacademies.org/fnb/food-and-nutrition-board |
Key Takeaways
- The World Health Organizations defines health as “a state of complete physical, mental, and social well-being, and not merely the absence of disease or infirmity.”
- Disease is defined as any abnormal condition that affects the health of an organism, and is characterized by specific signs and symptoms.
- Good nutrition provides a mechanism to promote health and prevent disease.
- Assessing your nutritional health using the ABCDEF characteristics can help identify risk factors for disease and encourage changes that could lead to improved health.
- Nutrient deficiencies can either be primary or secondary.
- Nutrients are classified based on the amounts required for proper body functioning. Macronutrients (carbohydrates, protein, lipids, and water) are needed in relatively large amounts, and micronutrients (vitamins and minerals) are needed in very small amounts.
- Food and/or meal quality can be measured based on its nutrient density and its energy density.
- The scientific method is an organized process of inquiry used in nutritional science to determine if the food suspect fits the claim and is part of the overall evidence-based approach to designing nutritional guidelines that are based on facts.
- There are different types of scientific studies—epidemiological studies, randomized clinical interventional trial studies, and laboratory animal and cell studies—which all provide different, complementary lines of evidence.
- It takes time to build scientific evidence that culminates as a commonly accepted conclusion.
- Reliable nutritional news will be based upon solid scientific evidence, supported by multiple studies, and published in peer-reviewed journals.
Portions of this chapter were taken from OER Sources listed below:
Tharalson, J. (2019). Nutri300:Nutrition. https://med.libretexts.org/Courses/Sacremento_City_College/SSC%3A_Nutri_300_(Tharalson)
Titchenal, A., Calabrese, A., Gibby, C., Revilla, M.K.F., 7 Meinke, W. (2018). Human Nutrition. University of Hawai’i at Manoa Food Science and Human Nutrition Program Open Textbook. https://pressbooks.oer.hawaii.edu
Zimmerman, M., & Snow, B. (2012). An Introduction to Nutrition, v. 1.0. https://2012books.lardbucket.org/books/an-introduction-to-nutrition/
Additional References:
- World Health Organization. (1946). Preamble to the Constitution of the World Health Organization as adopted by the International Health Conference. Official Records of the World Health Organization. https://www.who.int/about/who-we-are/constitution
- Xu, J., Murphy, S. L., Kochanek, K. D., & Arias, E. (2020). Mortality in the United States, 2018. National Center for Health Statistics. Data brief, no 355. https://www.cdc.gov/nchs/products/databriefs/db355.htm
- Klemm, S. (2019, July 15). Functional foods. Academy of Nutrition and Dietetics. https://www.eatright.org/food/nutrition/healthy-eating/functional-foods
- Harvard Health Letter. (2019, February). Fill up on phytochemicals. Harvard Medical School. https://www.health.harvard.edu/staying-healthy/fill-up-on-phytochemicals
- Zimmerman, M. B. (2008). Research on iodine deficiency and goiter in the 19th and early 20th centuries. The Journal of Nutrition, 138(11), 2060-63. doi:10.1093/jn/138.11.2060
- Carpenter, K. J. (2005). David Marine and the problem of goiter. The Journal of Nutrition, 135(4), 675-80. https://doi:10.1093/jn/135.4.675
- Briss, P.A., Zaza, S., Pappaioanou, M., Fielding, J., Wright-De Agüero, L., Truman, B. I., Hopkins, D, P., Mullen, P. D., Thompson, R. S., Woolf, S. H., Carande-Kulis, V. G., Anderson, L., Hinman, A. R., McQueen, D. V., Teutsch, S. M., & Harris, J. R. (2000). Developing an evidence-based guide to community preventive services-Methods. American Journal of Preventive Medicine, 18(1S), 35-43. https://doi:10.1016/s0749-3797(99)00119-1
- Johns Hopkins University. (2018). Reliable health information on the internet. https://www.hopkinsmedicine.org/johns_hopkins_bayview/_docs/patient_visitor_amenities/libraries/reliable_health_information_fall_2018.pdf
- Health on the Net. (2020, March). https://www.hon.ch/en/
- Utilization Review Accreditation Commission. (2020). Health website accreditation. https://www.urac.org/programs/health-web-site-accreditation
Media Attributions
- Figure 1.3.1 macros
- FEA72949-ECE3-489F-BBF8-BE1EC549BE43_4_5005_c
- 0367C105-FE04-4BDD-B2F0-6357E9FB090B
- 0BF8C415-BF38-4CB2-B614-E809A3882EC8
- Powdered-sugar raised donuts
- Healthy Breakfast Eggs Free Photo
- 011F2C6A-1E59-46BE-8287-A0DF9E333FF5
"A healthy outside starts from the inside."
-Robert Urich (1946-2002), American actor
Human bodies change significantly over time, and food is the fuel for those changes. People of all ages need the same basic nutrients—amino acids, carbohydrates, fatty acids, vitamins and minerals, water—to sustain life and health. However, the amounts of nutrients needed differ. Throughout the human life cycle, the body constantly changes and goes through different periods known as stages. In this chapter we will discuss the major changes that occur during each stage, focusing on the roles nutrition plays. The major stages of the human life cycle are defined as follows:
- Pregnancy. The development of a zygote into an embryo and then into a fetus in preparation for childbirth.
- Infancy. The earliest part of childhood. It is the period from birth through age 1.
- Toddler years. Occur during ages 2 and 3 and are the end of early childhood.
- Childhood. Takes place from ages 4 to 8.
- Puberty. The period from ages 9 to 13, which is the beginning of adolescence.
- Older adolescence. The stage that takes place between ages 14 and 18.
- Adulthood. The period from adolescence to the end of life. Begins at age 19.
- Middle age. The period of adulthood that stretches from age 31 to 50.
- Senior years, or old age. Extends from age 51 until the end of life.
Learning Objectives
- Summarize prenatal nutritional requirements and dietary recommendations.
- Discuss the most important nutritional concerns during pregnancy.
- Discuss the benefits and barriers related to breastfeeding.
- Examine feeding problems that parents and caregivers may face with their infants.
- Explore the introduction of solid foods into a toddler’s diet.
- Discuss the most important nutrition-related concerns during childhood.
- Discuss the most important nutrition-related concerns during adolescence.
- Explain how nutritional and lifestyle choices can affect current and future health.
- Discuss the most important nutrition-related concerns during middle and old age.
18.1 Pregnancy
Conception to the Early Days of Pregnancy
Women who are trying to conceive should make proper dietary choices and practice healthy habits to ensure the delivery of a healthy baby. Fathers-to-be should also consider their lifestyles. For both men and women, a sedentary lifestyle, excess body weight, and a diet low in fresh fruits and vegetables may affect fertility. Men who consume too much alcohol, use certain drugs, and/or smoke cigarettes/use tobacco may also damage the quantity and quality of their sperm.1 For both men and women, adopting healthy habits also boosts general well-being and makes it possible to meet the demands of parenting.
Pregnancy is measured from the first day of a woman’s last menstrual period until childbirth, and typically lasts about 40 weeks. Humans like to think of pregnancy in terms of equal time, so we divide pregnancy into three approximately equal sections or trimesters. The first trimester is the first 13 weeks of pregnancy, the second is weeks 14 through 27, and pregnancy ends with the third trimester, weeks 28 through birth.
However, trimesters do not reflect the actual stages of development through the pregnancy. The first trimester encompasses several stages of development. At conception, a sperm cell fertilizes an egg cell, creating a zygote. This first stage of pregnancy accounts for the first 2 weeks. The zygote rapidly divides into multiple cells to become an embryo and implants itself in the uterine wall. Major changes begin to occur in these earliest days after conception, often weeks before a woman even knows that she is pregnant. The embryonic stage lasts from week 3 through week 10. During this time there are critical periods of development where the infrastructure for organ systems such as the nervous system, heart, limbs, ears, eyes, teeth, palate, and external genitalia is laid down. During these periods the developing embryo is very sensitive to damage caused by inadequate nutrition, medications, alcohol, or exposure to other harmful substances. Adequate nutrition supports cell division, tissue differentiation, and organ development, especially during these critical times. As each week passes, new milestones are reached. The end of the embryonic stage marks the start of the fetal stage which is week 11 through birth. During this stage the organ systems grow to maturity, and weight of the fetus increases from about 1 oz to about 7.5 lb. At the 20-week mark, physicians typically perform an ultrasound to acquire information about the fetus and check for abnormalities. By this time, it is possible to know the sex of the baby.
Good nutrition is vital for any pregnancy and not only helps an expectant mother remain healthy, but also impacts the development of the fetus and ensures that the baby thrives in infancy and beyond. During pregnancy, a woman’s needs increase for certain nutrients more than for others. If these nutritional needs are not met, infants could suffer from low birth weight (a birth weight less than 5.5 lb, or 2,500 grams), among other developmental problems. Therefore, it is crucial to make careful dietary choices.
Weight Gain during Pregnancy
During pregnancy, a mother’s body changes in many ways. One of the most notable and significant changes is weight gain. If a pregnant woman does not gain enough weight, her unborn baby will be at risk. Infant birth weight is one of the best indicators of a baby’s future health. Poor weight gain by the mother, especially in the third trimester, could result not only in low birth weight, but also in infant intellectual disabilities or mortality. Therefore, it is vital for a pregnant woman to maintain a healthy weight, and her weight prior to pregnancy also has a major effect. Pregnant women at a healthy weight pre-pregnancy should gain between 25-35 lb in total through the entire pregnancy. The precise amount that a mother should gain usually depends on her beginning body mass index (BMI).
Table 18.1.1 Recommended Weight Gain During Pregnancy
| Pre-Pregnancy BMI | Weight Category | Recommended Weight Gain |
| < 18.5 | Underweight | 28-40 lb |
| 18.5-24.9 | Healthy | 25-35 lb |
| 25.0-29.9 | Overweight | 15-25 lb |
| > 30.0 | Obese (all classes) | 11-20 lb |
Starting weight below or above the healthy range can lead to different complications. Pregnant women with a pre-pregnancy BMI below 20 kg/m2 are at a higher risk of a preterm delivery and an underweight infant. Pregnant women with a pre-pregnancy BMI above 30 kg/m2 have an increased risk of the need for a cesarean section during delivery. Therefore, it is optimal to have a BMI in the normal range prior to pregnancy.
Generally, women gain 2 to 5 lb in the first trimester. After that, it is recommended to gain no more than one lb per week until birth. Some of the new weight is due to the growth of the fetus, while some is due to changes in the mother’s body that support the pregnancy. Weight gain often breaks down in the following manner: 6 to 8 lb of fetus, 1 to 2 lb for the placenta (which supplies nutrients to the fetus and removes waste products), 2 to 3 lb for the amniotic sac (which contains fluids that surround and cushion the fetus), 1 to 2 lb in the breasts, 1 to 2 lb in the uterus, 3 to 4 lb of maternal blood, 3 to 4 lb maternal fluids, and 8 to 10 lb of extra maternal fat stores that will be needed for breastfeeding and delivery for a total of 25-35 lb. Women who are pregnant with more than one fetus are advised to gain even more weight to ensure the health of their unborn babies.

Weight Loss after Pregnancy
During labor, new mothers lose some of their gained weight (usually 9-13 lb) with the delivery of their child (weight of the baby, the placenta, and the amniotic fluid). In the following weeks, they continue to shed weight as they lose accumulated fluids and their blood volume returns to normal. Some studies have found that exclusive breastfeeding helps a new mother lose some of the extra weight when compared to non-exclusive breastfeeding.2
New mothers who gain the recommended amount of weight and participate in regular physical activity during their pregnancies have an easier time shedding weight post-pregnancy. However, women who gain more weight than needed for a pregnancy typically retain that excess weight as body fat. If that weight gain increases a new mother’s BMI by a unit or more, that could lead to complications such as hypertension or gestational diabetes in future pregnancies and later in life.
Nutritional Requirements
As a mother’s body changes, so do her nutritional needs. Pregnant women must consume more kcal and nutrients in the second and third trimesters than other adult women. However, the average recommended daily caloric intake can vary depending on activity level and the mother’s normal weight. Regardless, pregnant women should choose a high quality, diverse diet, consume fresh foods, and nutrient-rich meals. It is also standard for pregnant women to take prenatal supplements to ensure adequate intake of necessary micronutrients.
Energy and Macronutrients
During the first trimester, a pregnant woman has the same energy requirements as normal and should consume the same number of kcal as usual. However, as the pregnancy progresses, a woman must increase her caloric intake. A pregnant woman should consume an additional 340 kcal per day during the second trimester, and an additional 450 kcal per day during the third trimester.3 This is partly due to an increase in metabolism which rises during pregnancy. A woman can easily meet these increased needs by consuming more nutrient dense foods.
The recommended dietary allowance, or RDA, of carbohydrates during pregnancy is about 175 to 265 g per day to fuel fetal brain development. The best food sources for pregnant women include whole grain breads and cereals, brown rice, whole vegetables, legumes, and fruits. These and other unrefined carbohydrates provide nutrients, phytochemicals, antioxidants, and the extra 3 mg/day of fiber that is recommended during pregnancy. These foods also help to build the placenta and supply energy for the growth of the unborn baby.
During pregnancy, extra protein is needed for the synthesis of new maternal and fetal tissues. Protein builds muscle and other tissues, enzymes, antibodies, and hormones in both the mother and the unborn baby. Additional protein also supports increased blood volume and the production of amniotic fluid. Protein should be derived from healthy sources, such as lean red meat, poultry, legumes, nuts, seeds, eggs, and fish. Low-fat milk and other dairy products also provide protein, along with calcium and other micronutrients. To calculate protein needs during pregnancy, use pre-pregnancy weight in kg body weight times the RDA for protein (0.8 g/kg/day), and add 25 g. For example, if your pre-pregnancy weight was 150 lb:
- Convert 150 lb to kg by dividing by 2.2: 150 lb ÷ 2.2 lb/kg = 68 kg
- Multiply 68 kg by RDA: 68 kg x 0.8 g/kg/day = 54.5 g protein
- Add 25 g during second and third trimester: 54.5 g + 25 g = ~80 g protein
There are no specific recommendations for fats in pregnancy, apart from following normal dietary guidelines. However it is recommended to increase the amount of essential fatty acids (omega-3 and omega-6) because they are incorporated into the placenta and fetal tissues. Fats should make up 25-35% of daily kcal and should come from healthy sources, such as avocados, nuts and nut butters, and olives and olive oils. It is not recommended for pregnant women to be on a very low-fat diet, since it would be hard to meet the needs of essential fatty acids and fat soluble vitamins. Fatty acids are important during pregnancy because they support the baby’s brain and eye development.
Fluids
Fluid intake must also be monitored. According to the National Academy of Medicine (NAM), pregnant women should drink at least 2.3 liters (about 10 cups) of liquids per day to provide enough fluid for blood production.4 It is also important to drink additional liquids during physical activity or when it is hot and humid outside, to replace fluids lost via perspiration. The combination of a high fiber diet and lots of liquids also helps to eliminate waste.
Vitamins and Minerals
The daily requirements for women change with the onset of a pregnancy. Taking a daily prenatal supplement or multivitamin helps to meet many nutritional needs. However, most of these requirements should be fulfilled with a healthy diet. The following table compares the non-pregnant levels of required vitamins and minerals to the levels needed during pregnancy. For pregnant women, the RDA of nearly all vitamins and minerals increases.
Table 18.1.2 Recommended Micronutrient Intakes during Pregnancy
| Nutrient | Non-Pregnant Women | Pregnant Women |
| Vitamin A (mcg) | 700.0 | 770.0 |
| Thiamin (mg) | 1.1 | 1.4 |
| Riboflavin (mg) | 1.1 | 1.4 |
| Niacin (mg) | 14.0 | 18.0 |
| Vitamin B6 (mg) | 1.3 | 1.9 |
| Folate (mcg) | 400.0 | 600.0 |
| Vitamin B12 (mcg) | 2.4 | 2.6 |
| Vitamin C (mg) | 75.0 | 85.0 |
| Vitamin D (mcg) | 15.0 | 15.0 |
| Vitamin E (mg) | 15.0 | 15.0 |
| Calcium (mg) | 1000.0 | 1000.0 |
| Iron (mg) | 18.0 | 27.0 |
| Magnesium (mg) | 310.0 (19-30 yr) | 350.0 (19-30 yr) |
| 320.0 (31-50 yr) | 360.0 (31-50 yr) | |
| Phosphorus (mg) | 700.0 | 700.0 |
| Zinc (mg) | 8.0 | 11.0 |
The micronutrients involved with building the skeleton—vitamin D and calcium—are crucial during pregnancy to support fetal bone development. Although the recommended levels are the same as those for non-pregnant women, many women do not typically consume adequate amounts and should make an extra effort to meet those needs.
There is an increased need for all B vitamins during pregnancy. Adequate vitamin B6 supports the metabolism of amino acids, while more vitamin B12 is needed for the synthesis of red blood cells and DNA. Additional zinc is crucial for cell development and protein synthesis. The need for vitamin A also increases, and extra iron intake is important because of the increase in blood supply during pregnancy and to support the fetus and placenta. Iron needs increase by 1/3, and this increase is almost impossible to obtain in adequate amounts from food sources during pregnancy. Therefore, even if a pregnant woman consumes a healthy diet, there may still be a need to take an iron supplement, in the form of ferrous salts. Also remember that folate needs increase during pregnancy to 600 mcg per day to prevent neural tube defects (during the first 8 weeks of pregnancy). This micronutrient is also crucial because it helps produce the extra blood a woman’s body requires during pregnancy.
For other micronutrients, recommended intakes are the same as those for non-pregnant women, although it is crucial for pregnant women to make sure to meet the RDAs to reduce the risk of birth defects. In addition, pregnant mothers should avoid exceeding any recommendations. Taking megadose supplements can lead to excessive amounts of certain micronutrients, such as vitamin A and zinc, which may produce toxic effects that can also result in birth defects.
Guide to Eating during Pregnancy
Almost all of the modified energy and nutrient needs required during pregnancy can be met by consuming nutrient dense foods, which are essential to a healthy diet. Examples of nutrient dense foods include fruits, vegetables, whole grains, peas, beans, reduced-fat dairy, and lean meats. Pregnant women should be able to meet almost all of their increased needs via a healthy diet. However, as discussed previously, expectant mothers should take a prenatal supplement to ensure an adequate intake of iron and folate. Here are some additional dietary guidelines for pregnant women4:
- Eat iron-rich or iron-fortified foods, including meat or meat alternatives, breads, and cereals, to help satisfy increased need for iron and prevent anemia. Include vitamin C-rich foods, such as orange juice, broccoli, or strawberries, or peppers to enhance iron absorption.
- Eat a well-balanced diet including fruits, vegetables, whole grains, calcium-rich foods, lean meats, and a variety of cooked seafood (excluding fish that are high in mercury, such as swordfish and shark).
- Drink additional fluids, especially water.
Foods to Avoid
A number of substances can harm a growing fetus. Therefore, it is vital for women to avoid them throughout a pregnancy. Some are so detrimental that a woman should avoid them even if she suspects that she might be pregnant. For example, consumption of alcoholic beverages results in a range of abnormalities that fall under the umbrella of Fetal Alcohol Spectrum Disorders. They include learning and attention deficits, heart defects, and abnormal facial features. Alcohol enters the unborn baby via the umbilical cord and can slow fetal growth, damage the brain, or even result in miscarriage. The effects of alcohol are most severe in the first trimester, when the organs are developing. As a result, there is no safe amount of alcohol that a pregnant woman should consume.
Pregnant women should also limit caffeine intake, which is found not only in coffee, but also tea, colas, cocoa, chocolate, and some over-the-counter painkillers. Some studies suggest that very high amounts of caffeine have been linked to babies born with low birth weights. Most experts agree that small amounts of caffeine each day are safe for most pregnant women (approximately 200 mg/day or less)5 but check with your doctor.
For both mother and child, foodborne illness can cause major health problems. For example, the foodborne illness caused by the bacteria Listeria monocytogenes can cause spontaneous abortion and fetal or newborn meningitis. According to the Centers for Disease Control and Prevention (CDC), pregnant women are 10 times more likely to become infected with this disease than non-pregnant, healthy adults.6 Foods more likely to contain the bacteria and that should be avoided include unpasteurized dairy products, especially soft cheeses, smoked seafood, hot dogs, paté, cold cuts, and uncooked meats.
Pregnant women can eat fish, ideally 8 to 12 oz of different types each week. Expectant mothers are able to eat cooked shellfish such as shrimp, farm-raised fish such as salmon, and a maximum of 6 oz of albacore or white, tuna per week. However, they should avoid fish with high methylmercury levels, such as shark, swordfish, and king mackerel. (Please refer to Table 3.3.2 Mercury Levels in Fish in Chapter 3). Pregnant women should also avoid consuming raw fish to avoid foodborne illness.
Food Cravings and Aversions
Food aversions and cravings can occur during pregnancy and often get a lot of attention. Fortunately most do not have a major impact unless food choices are extremely limited. For most women, it is not harmful to indulge in the occasional craving, such as a desire for pickles and ice cream. However, a medical disorder known as pica, the craving and willing consumption of substances with little or no nutritive value, such as dirt, clay, or laundry starch, can be harmful. Pica is most prevalent among pregnant women and young children. Although the etiology (or cause) of pica is not completely understood, several studies have linked pica, particularly during pregnancy, to iron deficiency anemia.7
Physical Activity during Pregnancy
For most pregnant women, physical activity is a must and is recommended in the 2020 Dietary Guidelines for Americans. Regular exercise of moderate intensity, about 30 minutes per day most days of the week, keeps the heart and lungs healthy. It also helps to improve sleep and boosts mood and energy levels. In addition, women who exercise during pregnancy report fewer discomforts and may have an easier time losing excess weight after childbirth. Brisk walking, swimming, or an aerobics class geared toward expectant mothers are all great ways to get exercise during a pregnancy. Healthy women who already participate in vigorous activities, such as running, can continue doing so during pregnancy provided they discuss their exercise plan with their physicians.
However, pregnant women should avoid activities that could cause injury, such as soccer, football, and other contact sports, or activities that could lead to falls, such as horseback riding and downhill skiing. It may be best for pregnant women not to participate in certain sports, such as tennis, that require you to jump or change direction quickly. Scuba diving should also be avoided because it might result in the fetus developing decompression sickness.
Complications during Pregnancy
Expectant mothers may face different complications during the course of their pregnancy. They include certain medical conditions that could greatly impact a pregnancy if left untreated, such as gestational hypertension and gestational diabetes, which have diet and nutrition implications.
Gestational Hypertension
Gestational hypertension is a condition of high blood pressure during the second half of pregnancy. First time mothers are at a greater risk, along with women who have mothers or sisters who had gestational hypertension, women carrying multiple fetuses, women with a prior history of high blood pressure or kidney disease, and women who are overweight or obese when they become pregnant. Hypertension can prevent the placenta from getting enough blood, which would result in the baby getting less oxygen and nutrients. This can result in low birth weight, although most women with gestational hypertension can still deliver a healthy baby if the condition is detected and treated early.
Some risk factors for gestational hypertension can be controlled such as diet, while others cannot, such as family history. If left untreated, gestational hypertension can lead to a serious complication called preeclampsia, which is sometimes referred to as toxemia. This disorder is marked by elevated blood pressure, protein in the urine, and is associated with fluid retention and swelling. If preeclampsia worsens, a life-threatening condition for both the mother and the baby called eclampsia can occur.
Gestational Diabetes
About 8% of pregnant women suffer from a condition known as gestational diabetes, or abnormal glucose tolerance during pregnancy.8 As discussed in Chapter 5, gestational diabetes is similar to type 2 diabetes. The mother's body becomes resistant to the hormone insulin, which enables cells to transport glucose from the blood and into cells. Gestational diabetes is typically diagnosed between 24-28 weeks using a glucose tolerance test, although it is possible for the condition to develop later into a pregnancy. Signs and symptoms include extreme hunger, thirst, or fatigue. The excess glucose in the mother's blood is transported to the placenta, and the fetus will take up this excess glucose from the mother. If blood glucose levels are not properly monitored and treated, the baby might gain too much weight, possibly causing a premature birth and/or a difficult delivery. Diet and regular physical activity can help to manage this condition. Some patients with gestational diabetes may require daily insulin injections to boost the absorption of glucose from the bloodstream and promote the storage of glucose in the form of glycogen in liver and muscle cells. Gestational diabetes usually resolves quickly after childbirth, however women who suffer from this condition have a 50% chance of eventually developing type 2 diabetes later in life, particularly if they are overweight.
18.2 Breastfeeding
After the birth of the baby, nutritional needs must be met to ensure that an infant not only survives, but thrives from infancy into childhood. Exclusive breastfeeding is one of the best ways a mother can support the growth and protect the health of her infant child.
Breast milk contains all of the nutrients that a newborn requires for rapid growth and development and gives a child the best start to a healthy life. New mothers must consider their own nutritional requirements to help their bodies recover in the wake of the pregnancy and delivery. This is particularly true for women who breastfeed their babies, which calls for an increased intake of certain nutrients.
Benefits of Breastfeeding
 Breastfeeding has a number of benefits, both for the mother and for the child. Breast milk contains immunoglobulins, enzymes, immune factors, and white blood cells. As a result, breastfeeding boosts the baby’s immune system and lowers the incidence of diarrhea, along with respiratory diseases, gastrointestinal problems, and ear infections. Breastfed babies also are less likely to develop asthma and allergies, and breastfeeding lowers the risk of sudden infant death syndrome (SIDS). In addition, human milk encourages the growth of healthy bacteria in an infant’s intestinal tract. All of these benefits remain in place long after an infant has been weaned from breast milk. Some studies suggest other possible long-term effects. For example, breast milk may protect against type 1 diabetes and obesity, although research is ongoing in these areas.9
Breastfeeding has a number of benefits, both for the mother and for the child. Breast milk contains immunoglobulins, enzymes, immune factors, and white blood cells. As a result, breastfeeding boosts the baby’s immune system and lowers the incidence of diarrhea, along with respiratory diseases, gastrointestinal problems, and ear infections. Breastfed babies also are less likely to develop asthma and allergies, and breastfeeding lowers the risk of sudden infant death syndrome (SIDS). In addition, human milk encourages the growth of healthy bacteria in an infant’s intestinal tract. All of these benefits remain in place long after an infant has been weaned from breast milk. Some studies suggest other possible long-term effects. For example, breast milk may protect against type 1 diabetes and obesity, although research is ongoing in these areas.9
Breastfeeding has a number of other important benefits. It is easier for babies to digest breast milk than bottle formula, which often contains proteins made from cow’s milk that require an adjustment period for infant digestive systems. Breastfed infants are sick less often than formula-fed infants. Breastfeeding is more sustainable and results in less plastic waste and other trash. Breastfeeding can also save families money because it does not incur the same cost as purchasing formula. Breast milk is always ready. It does not have to be mixed, heated, or prepared. Also, breast milk is sterile and always at the right temperature. In addition, the skin-to-skin contact of breastfeeding promotes a close bond between mother and baby, which provides important emotional and psychological benefits. The practice also provides health benefits for the mother. Studies have shown that breastfeeding reduces the risk of type 2 diabetes, and breast and ovarian cancers for the mother.9
The choice to breastfeed is one that all new mothers face. Although breast milk is ideal for almost all infants, there are some challenges that nursing mothers may face when starting and continuing to breastfeed their infants. These obstacles include painful engorgement or fullness in the breasts, sore and tender nipples, lack of comfort or confidence in public, and lack of accommodation to breastfeed or express milk in the workplace. Support from family members, friends, employers, and others can greatly help with both the decision making process during pregnancy and the practice of breastfeeding after the baby’s birth. In the US in 2015, about 83% of babies started out being breastfed. Yet by the age of six months, when solid foods should begin to be introduced, only 24% of infants were still breastfed exclusively. Employed mothers have been less likely to initiate breastfeeding and tend to breastfeed for a shorter period of time than new mothers who are not employed outside the home or who have lengthy maternity leaves.10 Around the world, less than 40% of infants under the age of six months are breastfed exclusively.11
International Board Certified Lactation Consultants are healthcare professionals (often a registered nurse or registered dietitian) certified in breastfeeding management that work with new mothers to solve problems and educate families about the benefits of this practice. Women who give birth in hospitals with lactation consultants are more likely to breastfeed. Once a new mother has left the hospital for home, she also needs access to a trained individual who can provide consistent information.12 Lactation consultants can help new mothers learn proper technique, and help troubleshoot breastfeeding problems when they occur.
Affordable Care Act and Breastfeeding
In 2010 in the US, the passage of the Affordable Care Act (ACA) called for employers to provide accommodations within the workplace for new mothers to pump breast milk. This law requires a private and clean space within the workplace, other than a restroom, along with adequate break time for a woman to express milk. Yet as of 2018 only 49% of employers provided worksite lactation support programs.10
Contraindications to Breastfeeding
Although there are numerous benefits to breastfeeding, in some cases there are also risks that must be considered. A new mother with HIV should not breastfeed as the infection can be transmitted through breast milk. Breastfeeding is also not recommended for women undergoing radiation or chemotherapy treatment for cancer. Women actively using alcohol excessively and/or illicit drugs should also avoid breastfeeding.
Lactation
Lactation (or lactogenesis) is the synthesis and secretion of breast milk. An infant suckling at the breast stimulates nerve endings which signal the pituitary gland to release two hormones, prolactin and oxytocin. Prolactin signals the growth of the milk duct system and initiates and maintains milk production in the alveoli of the breast.
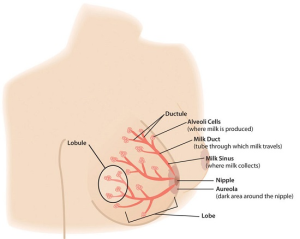
Oxytocin is involved in milk ejection, also called milk letdown. It signals contraction of the alveoli cells, forcing milk into the ducts and out through the nipple. The nipple tissue becomes firmer with stimulation, which makes it more flexible and easier for the baby to grasp in the mouth. The release of oxytocin also has psychological benefits by inducing calm and enhancing feelings of affection or bonding between mother and baby.13
New mothers need to adjust their caloric and fluid intake to make breastfeeding possible. The RDA is 330 additional kcal per day during the first six months of lactation and 400 additional kcal during the second six months of lactation. The energy needed to support breastfeeding comes from both increased intake and from stored fat. For example, during the first six months after her baby is born, the daily caloric cost for a lactating mother is 500 kcal, with 330 kcal derived from increased intake and 170 kcal derived from maternal fat stores. This helps explain why breastfeeding may promote weight loss in new mothers. Lactating women should also drink approximately 13 cups of liquids per day to maintain milk production, according to the NAM. As is the case during pregnancy, the RDA of several vitamins and minerals increases for women who are breastfeeding their babies. The following table compares the recommended vitamins and minerals for lactating women to the levels for non-pregnant and pregnant women.
Table 18.2.1 Recommended Micronutrient Intakes during Pregnancy
| Nutrient | Non-Pregnant Women | Pregnant Women | Lactating Women |
| Vitamin A (mcg) | 700.0 | 770.0 | 1300.0 |
| Thiamin (mg) | 1.1 | 1.4 | 1.4 |
| Riboflavin (mg) | 1.1 | 1.4 | 1.6 |
| Niacin (mg) | 14.0 | 18.0 | 17.0 |
| Vitamin B6 (mg) | 1.3 | 1.9 | 2.0 |
| Folate (mcg) | 400.0 | 600.0 | 500.0 |
| Vitamin B12 (mcg) | 2.4 | 2.6 | 2.8 |
| Vitamin C (mg) | 75.0 | 85.0 | 120.0 |
| Vitamin D (mcg) | 15.0 | 15.0 | 15.0 |
| Vitamin E (mg) | 15.0 | 15.0 | 19.0 |
| Calcium (mg) | 1000.0 | 1000.0 | 1000.0 |
| Iron (mg) | 18.0 | 27.0 | 9.0 |
| Magnesium (mg) | 310.0 (19-30 yr) | 350.0 (19-30 yr) | 310.0 (19-30 yr) |
| 320.0 (31-50 yr) | 360.0 (31-50 yr) | 320.0 (31-50 yr) | |
| Phosphorus (mg) | 700.0 | 700.0 | 700.0 |
| Zinc (mg) | 8.0 | 11.0 | 12.0 |
Calcium requirements do not change during breastfeeding because of more efficient absorption, which is the case during pregnancy, as well. However, the reasons for this differ. During pregnancy, there is enhanced absorption of calcium within the gastrointestinal tract. During lactation, there is enhanced retention by the kidneys. The RDA for phosphorus, vitamin D, and fluoride also remain the same. The RDA for iron is reduced significantly during lactation to half of the requirement for non-pregnant women. This is because, for most women, lactation significantly reduces or eliminates menstruation.
Components of Breast Milk
Human breast milk not only provides adequate and highly bioavailable nutrition for infants, it also helps to protect newborns from disease. Breast milk is rich in cholesterol, which is needed for brain development. Colostrum is produced immediately after birth, prior to the start of milk production, and lasts for several days after the arrival of the baby. Colostrum is thicker than breast milk, and is often yellowish in color. This protein-rich liquid fulfills an infant’s nutrient needs during those early days. Although low in volume, colostrum is packed with concentrated nutrition for newborns. This special "milk" is high in fat-soluble vitamins, minerals, and immunoglobulins (antibodies) that pass from the mother to the baby. Immunoglobulins provide passive immunity for the newborn and protect the baby from bacterial and viral diseases.14

Two to four days after birth, colostrum is replaced by transitional milk. Transitional milk is a creamy liquid that lasts for approximately two weeks and includes high levels of fat, lactose, and water soluble vitamins. It also contains more kcal than colostrum.
Mature milk is the final fluid that a new mother produces. In most women, this begins by the end of the second week postpartum. There are two types of mature milk that appear during a feeding. Foremilk occurs at the beginning and includes more water, vitamins, and protein. Hindmilk occurs after the initial release of milk and contains higher levels of fat, which is necessary for weight gain. Combined, these two types of milk ensure that a baby receives adequate nutrients to grow and develop properly.15
About 90% of mature milk is water, which helps an infant remain hydrated. The remaining 10% contains carbohydrates, proteins, and fats, which support energy and growth. Similar to cow’s milk, the main carbohydrate of mature breast milk is lactose. Breast milk contains vital essential fatty acids, such as docosahexaenoic acid (DHA) and arachidonic acid (ARA). In terms of protein, breast milk contains more whey than casein (which is the reverse of cow’s milk). Whey is much easier for infants to digest than casein. Complete protein, which means all of the essential amino acids, is also present in breast milk, as well as lactoferrin, an iron-gathering compound that helps to absorb iron into an infant’s bloodstream.
In addition, breast milk provides adequate vitamins and minerals. Although absolute amounts of some micronutrients are low, they are more efficiently absorbed by infants. Other essential components include digestive enzymes that help a baby digest the breast milk. Human milk also provides the hormones and growth factors that help a newborn to develop.
Diet and Milk Quality
A mother’s diet can have a major impact on milk production and quality. As during pregnancy, lactating mothers should avoid harmful substances such as tobacco. Some legal drugs and herbal products can be harmful as well, so it is important to discuss them with a healthcare provider. Some mothers may need to avoid certain things, such as spicy foods, that can produce gas in sensitive infants. Avoiding alcohol completely is the safest option for a breastfeeding mother. However, consumption of up to one alcoholic drink a day (12 oz of beer, 5 oz of wine, or 1.5 oz of liquor) is not known to be harmful to the infant, particularly if the mother waits 2-3 hours after consumption to breastfeed.16
In terms of the mother’s nutrient intake, there is limited research regarding the extent of its role on breast milk composition. A systematic review of 36 journal publications found that the concentration of fatty acids and vitamins A, C, B6, and B12 are reported to be most influenced by maternal diet, while mineral content is much less affected.17 However, more research on this topic is needed.
Bottle Formula Feeding
Most women can and should breastfeed when given sufficient education and support. However, as discussed, a small percentage of women are unable to breastfeed their infants, while others choose not to. While infant formula provides a balance of nutrients, not all formulas are the same and there are important considerations that parents and caregivers must weigh. Standard formulas use cow’s milk as a base. They have 20 kcal per fl oz, similar to breast milk, with vitamins and minerals added. Cow’s milk alone should never be given to babies under the age of one as young infants cannot fully digest it and it does not meet their nutrient needs. Soy-based formulas are usually given to infants who develop diarrhea, constipation, vomiting, colic, or abdominal pain, or to infants with a cow’s milk protein allergy.
Hypoallergenic protein hydrolysate formulas are usually given to infants who are allergic to cow’s milk and soy protein. This type of formula uses hydrolyzed protein, meaning that the protein is already broken down into amino acids and small peptides, which makes it easier to digest. Preterm infant formulas are given to low birth weight infants, if breast milk is unavailable. Preterm infant formulas have 24 kcal per fl oz and are given until the infant reaches a desired weight.
Infant formula comes in three basic types:
- Powder that requires mixing with water. This is the least expensive type of formula.
- Concentrates, which are liquids that must be diluted with water. This type is slightly more expensive.
- Ready-to-use liquids that can be poured directly into bottles. This is the most expensive type of formula. However, it requires the least amount of preparation. Ready-to-use formulas are also convenient for traveling.
Most babies need about 2.5 oz of formula per lb of body weight each day. Therefore, the average infant should consume about 24 fl oz of breast milk or formula per day. When preparing formula, parents and caregivers should carefully follow the safety guidelines, since an infant has an immature immune system. All equipment used in formula preparation should be sterilized. Prepared, unused formula should be refrigerated to prevent bacterial growth. Parents should make sure not to use contaminated water to mix formula in order to prevent foodborne illnesses. Follow the instructions for powdered and concentrated formula carefully. Formula that is overly diluted would not provide adequate kcal and protein, while overly concentrated formula provides too much protein and too little water which can impair kidney function.
It is important to note again that both the American Academy of Pediatrics and the World Health Organization (WHO) state that breast milk is far superior to infant formula. This table compares some of the advantages of giving a child breast milk to the disadvantages of using bottle formula.
Table 18.2.2 Breast Milk vs. Bottle Formula
| Breast Milk | Bottle Formula |
| Antibodies and lactoferrin in breast milk protect infants. | Formula does not contain immunoprotective factors. |
| The iron in breast milk is absorbed more easily. | Formula contains more iron than breast milk but it is less easily absorbed. |
| The feces that breastfed babies produce lacks smell due to different bacteria in the gut. | The feces that formula fed infants produce tends to have more of a foul odor. |
| Breast milk is always available and is always at the correct temperature. | Formula must be prepared, refrigerated for storage and warmed before given to an infant. |
| Breastfed babies are less likely to have constipation. | Formula fed babies tend to have more constipation. |
| Breastfeeding ostensibly is free, though purchasing a pump and bottles to express milk does require some expense. | Formula must be purchased and is expensive. |
| Breast milk contains the essential fatty acids, DHA and ARA, which are critical for brain and vision development. | Some formulas contain DHA and ARA. |
18.3 Infancy
Diet and nutrition have a major impact on a child’s development from infancy into the adolescent years. A healthy diet not only affects growth, but also immunity, intellectual capabilities, and emotional well-being. One of the most important jobs of parenting is making sure that children receive an adequate amount of needed nutrients to provide a strong foundation for the rest of their lives.
Infant Growth and Development
A number of major physiological changes occur during infancy. The trunk of the body grows faster than the arms and legs, while the head becomes less prominent in comparison to the limbs. Organs and organ systems grow at a rapid rate. Also during this period, countless new synapses form to link brain neurons. Two soft spots on the baby’s skull, known as fontanels, allow the skull to accommodate rapid brain growth. The posterior fontanel closes first, by eight weeks of age. The anterior fontanel closes about a year later, at 18 months on average. Developmental milestones include sitting up without support, learning to walk, teething, and vocalizing among many, many others. All of these changes require adequate nutrition to ensure development at the appropriate rate.18
this period, countless new synapses form to link brain neurons. Two soft spots on the baby’s skull, known as fontanels, allow the skull to accommodate rapid brain growth. The posterior fontanel closes first, by eight weeks of age. The anterior fontanel closes about a year later, at 18 months on average. Developmental milestones include sitting up without support, learning to walk, teething, and vocalizing among many, many others. All of these changes require adequate nutrition to ensure development at the appropriate rate.18
Healthy infants grow steadily, but not always at an even pace. For example, during the first year of life, height increases by 50%, while weight triples. Physicians and other health professionals use growth charts to track a baby’s development process. Because infants cannot stand, length is used instead of height to determine the rate of a child’s growth. Other important developmental measurements include head circumference and weight. All of these must be tracked and compared against standard measurements for an infant’s age.
For infants and toddlers, the WHO growth charts are used to monitor growth. These standards represent optimal growth for children at this age and allow for tracking growth trends over time through percentile rankings. Growth charts may provide warnings that a child has a medical problem or is malnourished. Insufficient weight or height gain during infancy may indicate a condition known as failure-to-thrive, which is characterized by poor growth.
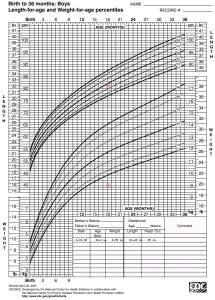
Nutritional Requirements
Requirements for macronutrients and micronutrients on a per kg basis are higher during infancy than at any other stage in the human life cycle. These needs are affected by the rapid cell division that occurs during growth, which requires energy and protein, along with the nutrients that are involved in DNA synthesis. During this period, children are entirely dependent on their parents or other caregivers to meet these needs. For almost all infants, six months or younger, breast milk is the best source to fulfill nutritional requirements. An infant may require feedings 8-12 times a day or more in the beginning. After six months, infants can gradually begin to consume solid foods to help meet nutrient needs.
Energy and Macronutrients
Energy needs relative to size are much greater in an infant than an adult. A baby’s resting metabolic rate is two times that of an adult. The RDA to meet energy needs changes as an infant matures and puts on more weight. Just as we calculate energy needs in adults using various equations, there are also equations to calculate total energy expenditure and resulting energy needs for infants and children. For example, the equation for the first three months of life is: (89 x weight [kg] − 100) + 175 kcal. However, the amount and frequency an infant wants to eat will also change over time due to growth spurts, which typically occur at about two and six weeks of age, and again at about three months and six months of age.
The dietary recommendations for infants are based on the nutritional content of human breast milk. Carbohydrates make up about 45-65% of the caloric content in breast milk, which amounts to an RDA of about 130 g. Almost all of the carbohydrate in human milk is lactose, which infants digest and tolerate well. In fact, lactose intolerance is practically nonexistent in infants (not to be confused with an allergy to the protein in cow's milk). Protein makes up about 5-20% of the caloric content of breast milk, which amounts to about 13 g per day. Infants need protein to support growth and development, though excess protein (which is only a concern with formula feeding) can cause dehydration, diarrhea, fever, and acidosis in premature infants. About 30-40% of the caloric content in breast milk is made up of fat. A high fat diet is necessary to encourage the development of neural pathways in the brain and other parts of the body. However, saturated fats and trans fatty acids inhibit this growth. Infants who are over the age of six months, which means they are no longer exclusively breastfed, should not consume foods that are high in these types of fats.
Micronutrients
Almost all of the nutrients that infants require can be met if they consume an adequate amount of breast milk. There are a few exceptions, though. Human milk is low in vitamin D, which is needed for calcium absorption and building bone, among other things. Therefore, breastfed children often need to take a vitamin D supplement in the form of drops. Infants at the highest risk for vitamin D deficiency are those with darker skin and/or no exposure to sunlight. Breast milk is also low in vitamin K, which is required for blood clotting, and deficits could lead to bleeding or hemorrhagic disease. Babies are born with limited vitamin K. Since 1961, the American Academy of Pediatrics has recommended newborns be given a low dose vitamin K injection shortly after birth.19
Breast milk is not high in iron, but the iron in breast milk is well absorbed by infants. Babies are born with about a six month supply of stored iron. After six months, however, an infant needs an additional source of iron other than breast milk. This is typically the time solid foods begin to be introduced, particularly iron-enriched cereals.20
Fluids
Infants have a high need for fluids, 1.5 ml per kcal consumed compared to 1.0 ml per kcal consumed for adults. This is because children have larger body surface area per unit of body weight and a reduced capacity for perspiration. Therefore, they are at greater risk of dehydration. However, parents or other caregivers can meet an infant’s fluid needs with breast milk or formula. As solids are introduced, parents must make sure that young children continue to drink fluids throughout the day.
Introducing Solid Foods
The American Academy of Pediatrics and the WHO recommends exclusive breastfeeding for the first six months of life, followed by continued breastfeeding as complementary foods are introduced, with continuation of breastfeeding for one year or longer as mutually desired by mother and infant.14
Infants should not exclusively consume solid foods prior to six months as these do not contain the right nutrient mix that infants need. If parents try to feed an infant who is too young or is not ready, their tongue will push the food out, which is called an extrusion reflex. Further, research suggests that infants who are fed solid foods too soon are more susceptible to developing food allergies. A child may be ready to eat solids, once they can sit with little or no support, has good head control, and opens their mouth and leans toward food when it is offered.20
Solid baby foods can be bought commercially or prepared from regular food using a food processor, blender, food mill, or grinder at home. By nine months to a year, infants are able to chew soft foods and can eat solids that are well chopped or mashed. It is important to feed a young child only one new food at a time, to help identify allergic responses or food intolerances. An iron supplement or iron-fortified cereal is still recommended at this time.
18.4 Toddler Years
Major physiological changes continue into the toddler years. Unlike in infancy, the limbs grow much faster than the trunk, which gives the body a more proportionate appearance. By the end of the third year, a toddler is taller and more slender than an infant, with a more erect posture. As the child grows, bone density increases and bone tissue gradually replaces cartilage.
Developmental milestones include running, drawing, toilet training, and self-feeding. How a toddler acts, speaks, learns, and eats offers important clues about their development. By the age of two, children have advanced from infancy and are on their  way to becoming school-aged children. Their physical growth and motor development slows compared to the progress they made as infants. However, toddlers experience enormous intellectual, emotional, and social changes. Of course, food and nutrition continue to play an important role in a child’s development. During this stage, the diet completely shifts from breastfeeding or formula feeding to solid foods along with other liquids. Parents of toddlers also need to be mindful of certain nutrition-related issues that may crop up during this stage of the human life cycle. For example, fluid requirements relative to body size are higher in toddlers than in adults because children are at greater risk of dehydration.
way to becoming school-aged children. Their physical growth and motor development slows compared to the progress they made as infants. However, toddlers experience enormous intellectual, emotional, and social changes. Of course, food and nutrition continue to play an important role in a child’s development. During this stage, the diet completely shifts from breastfeeding or formula feeding to solid foods along with other liquids. Parents of toddlers also need to be mindful of certain nutrition-related issues that may crop up during this stage of the human life cycle. For example, fluid requirements relative to body size are higher in toddlers than in adults because children are at greater risk of dehydration.
The toddler years pose interesting challenges for parents or other caregivers, as children learn how to eat on their own and begin to develop personal preferences.
Nutritional Requirements
A toddler’s serving sizes should be approximately one-quarter that of an adult serving size. One way to estimate serving sizes for young children is one tablespoon for each year of life. For example, a 2 year old child would be served 2 tbsp of fruits or vegetables at a meal, while a 4 year old would be given 4 tbsp, or one-quarter cup. Here is an example of a toddler-sized meal:
- 1 oz of meat or chicken, or 2 to 3 tbsp of beans
- 1/4 slice of whole-grain bread
- 1 to 2 tbsp of cooked vegetable
- 1 to 2 tbsp of fruit
Energy
The energy requirements for ages two to three are about 1,000-1,400 kcal a day. In general, a toddler needs to consume about 40 kcal for every inch of height. For example, a young child who measures 32 inches should take in an average of 1,300 kcal a day. However, the recommended caloric intake varies with each child’s level of activity. Toddlers require small, frequent, nutritious snacks and meals to satisfy energy requirements. The amount of food a toddler needs from each food group depends on daily kcal needs. See Table 18.4.1 for serving size guidelines.
Table 18.4.1 Serving Sizes for Toddlers21
| Food Group | 2 Year olds | 3 Year olds | What Counts as: |
| Fruit | 1 c | 1-1½ c | ½ cup of fruit?
|
| Vegetables | 1 c | 1-1½ c | ½ cup of veggies?
|
| Grains | 3 oz | 3-5 oz | 1 oz grain?
|
| Protein Foods | 2 oz | 2-4 oz | 1 oz protein food?
|
| Dairy | 2 c | 2-2½ c | ½ cup dairy?
|
Macronutrients
Toddlers’ needs increase to support their body and brain development. For toddlers, the AMDR for carbohydrate intake is 45-65% of daily kcal. For protein, it's 5-20% and for fat it's 30-40% of daily kcal. Essential fatty acids are vital for the development of the eyes, along with nerves and other types of tissue. However, toddlers should not consume foods with high amounts of trans fats and saturated fats. Instead, young children require the equivalent of three teaspoons of healthy oils, such as olive oil, each day.
Micronutrients
As a child grows bigger, the demands for micronutrients increase. These needs for vitamins and minerals can be met with a balanced diet, with a few exceptions. According to the American Academy of Pediatrics, toddlers and children of all ages need 15 mcg of vitamin D per day. Vitamin D-fortified milk and cereals can help to meet this need. However, toddlers who do not get enough of this micronutrient should receive a supplement. Pediatricians may also prescribe a fluoride supplement for toddlers who live in areas with fluoride-poor water.
Iron deficiency is also a major concern for children between the ages of two and three. Iron deficiency anemia (IDA) can cause a number of problems including weakness, pale skin, shortness of breath, fatigue, and irritability. It can also result in intellectual, behavioral, or motor problems. IDA can occur as young children are weaned from iron-rich foods, such as breast milk and iron-fortified formula. They begin to eat solid foods that may not provide enough of this nutrient. Therefore, it is important that parents and caregivers add more iron-rich foods to a child’s diet, including lean meats, fish, poultry, eggs, legumes, and iron-enriched whole-grain breads and cereals. Children may also be given a daily supplement, such as ferrous sulfate drops.
Food-Related Problems in the Toddler Years
During the toddler years, parents may face a number of problems related to food and nutrition. Possible obstacles include difficulty helping a young child overcome a fear of new foods, or fights over messy habits at the dinner table. Even in the face of problems and confrontations, parents and other caregivers must make sure their preschooler has nutritious choices at every meal. For example, even if a child stubbornly resists eating vegetables, parents should continue to provide them. Before long, the child may change their mind, and develop a taste for foods once abhorred. It is important to remember this is the time to establish or reinforce healthy habits.
Registered Dietitian Ellyn Satter states that feeding is a responsibility that is split between parent and child. According to Satter and her Division of Responsibility in Feeding, parents are responsible for what their infants eat, while infants are responsible for how much they eat. In the toddler years and beyond, parents are responsible for what children eat, when they eat, and where they eat, while children are responsible for how much food they eat and whether they eat. Satter states that the role of a parent or a caregiver in feeding includes the following22:
- selecting and preparing food
- providing regular meals and snacks
- making mealtimes pleasant
- showing children what they must learn about mealtime behavior
- being considerate of children's lack of food experiences without catering to likes and dislikes
Picky Eaters
Children at this stage are often picky about what they want to eat. They may turn their heads away after eating just a few bites. Or they may resist coming to the table at mealtimes. They also can be unpredictable about what they want to consume for specific meals or at particular times of the day. Although it may seem as if toddlers should increase their food intake to match their level of activity, there may be a good reason for picky eating. A child’s growth rate slows after infancy, and toddlers do not require as much food.
Some children may also go through a food jag, or period of time where they only want to eat the same few foods every day and for most, if not every, meal. While this can be a way for a child to begin to express some independence, which is a normal part of development, it can make for frustrating meal times. It's important not to force a child to eat foods they don't want as this can actually prolong the food jag. Instead, offer new foods or healthy foods that they like and allow them to eat the preferred food with remaining food on their plate. Remember to follow Ellyn Satter's Division of Responsibility in Feeding as stated above.
Choking
At this young age, children are still learning how to adequately chew and swallow, increasing the risk of choking. To minimize this risk, encourage children to sit when eating, chew thoroughly, play close attention to what they put in their mouths, and supervise older children who may give foods considered choking hazards to younger kids. Such foods include nuts, whole cherries or grapes, raw carrots or celery, hard candy, hot dogs, etc. Make sure to cut foods into smaller and/or mashed pieces.
Early Childhood Caries
Early childhood caries (dental issues such as cavities) remain a potential problem during the toddler years. The risk of early childhood caries increases with the consumption of foods with a higher sugar content. According to the National Health and Nutrition Examination Survey, children between ages of 2 and 5 consume slightly more than 200 kcal of added sugar per day or approximately 13% of their total kcal.26 This is much more than recommended. Therefore, parents with toddlers should avoid processed foods, such as snacks from vending machines, and sugary beverages, such as soda. Parents also need to instruct a child on brushing their teeth at this time to help a toddler develop healthy habits and avoid tooth decay.
Toddler Obesity
Another potential problem during the early childhood years is toddler obesity. According to the WHO, the number of overweight or obese infants and young children (five years and younger) has increased from 32 million globally in 1990 to 41 million in 2016.23 In the US, the proportion of obese two to five year-olds increased from 5% in the 1970s to 13.9% in 2015.24,25
Obesity during early childhood tends to linger as a child matures and can cause health problems later in life. Recall from Chapter 9 that children undergo both hyperplasia and hypertrophy of adipose tissue, and the additional adipose cells created during childhood remain in adulthood. There are a number of reasons for the increases in obesity rates in toddlers. One is a lack of time. Parents and other caregivers who are constantly on the go may find it difficult to fit home-cooked meals into a busy schedule and may turn to fast food and other conveniences that are quick and easy, but not nutritionally sound. Another contributing factor is a lack of access to fresh fruits and vegetables. This is a problem particularly in low-income neighborhoods where local stores and markets may not stock fresh produce or may have limited affordable options. Physical inactivity is also a factor, as toddlers who live a sedentary lifestyle are more likely to be overweight or obese. Another contributor is a lack of breastfeeding support. Children who were breastfed as infants show lower rates of obesity than children who were formula-fed.
To prevent or address toddler obesity parents and caregivers can do the following:
- Eat at the kitchen table instead of in front of a television to monitor what and how much a child eats.
- Offer a child healthy portions. The size of a toddler’s fist is an appropriate serving size.
- Toddlers should be physically active throughout the day, with no more than 60 minutes of sedentary activity, such as watching television, per day.
Food for Thought
What would you recommend to help families prevent obesity among their children? What tips would you provide? What lifestyle changes might help?
18.5 Childhood
Nutritional needs change as children leave the toddler years. From ages four to eight, school-aged children grow consistently, but at a slower rate than infants and toddlers. They also experience the loss of deciduous, or “baby” teeth, and the arrival of permanent "adult" teeth, which typically begins at age six or seven. As new teeth come in, many children have some malocclusion, or malposition, of their teeth, which may affect their ability to chew food. Other changes that affect nutrition include the influence of peers on dietary choices and the kinds of foods offered by schools and after-school programs, which can make up a sizable part of a child’s diet. Excessive weight gain early in life can lead to obesity into adolescence and adulthood.
At this life stage, a healthy diet facilitates physical and mental development and helps to maintain health and wellness. School-aged children experience steady, consistent growth, with an average growth rate of 2 to 3 inches in height and 4.5 to 6.5 lb in weight per year. In addition, the rate of growth for the extremities is faster than for the trunk, which results in more adult-like proportions.
Nutritional Requirements
Energy
Children’s energy needs vary depending on their growth and level of physical activity. Energy requirements may also vary according to biological sex. Girls ages 4 to 8 require 1,200-1,800 kcal a day, while boys need 1,200-2,000 kcal daily and, depending on their activity level, a child may require more. Also, recommended intakes of macronutrients and most micronutrients are higher relative to body size, compared with nutrient needs during adulthood.
Macronutrients
For carbohydrates, the AMDR remains 45-65% of daily kcal. Children also require 17-25 g of fiber per day. They have a high need for protein to support muscle growth and development, therefore the AMDR increases a bit to 10-30% of daily kcal. High levels of essential fatty acids are needed to support growth (although not as high as in infancy and toddler years). As a result, the AMDR for fat is 25-35% of daily kcal.
Micronutrients
Micronutrient needs should be met with foods first. Parents and caregivers should select a variety of foods from each food group to ensure that nutritional requirements are met. Because children grow rapidly, they require foods that are high in iron, such as lean meats, legumes, fish, poultry, and iron-enriched cereals. Adequate fluoride is crucial to support strong teeth. Two of the most important micronutrient requirements during childhood are adequate calcium and vitamin D intake. Both are needed to build dense bones and a strong skeleton. Children who do not consume adequate vitamin D should be given a supplement of 10 mcg per day. Table 18.5.1 shows the micronutrient recommendations for school-aged children. Note that the recommendations are the same for boys and girls. As we progress through the different stages of the human life cycle, there will be some differences between males and females regarding micronutrient needs.
Table 18.5.1 Recommended Micronutrient Intakes during Childhood
| Nutrient | 4-8 Years | 9-13 Years |
| Vitamin A (mcg) | 400.0 | 600.0 |
| Thiamin (mg) | 0.6 | 0.9 |
| Riboflavin (mg) | 0.6 | 0.9 |
| Niacin (mg) | 8.0 | 12.0 |
| Vitamin B6 (mg) | 0.6 | 1.0 |
| Folate (mcg) | 200.0 | 200.0 |
| Vitamin B12 (mcg) | 1.2 | 1.8 |
| Vitamin C (mg) | 25.0 | 45.0 |
| Vitamin D (mcg) | 15.0 | 15.0 |
| Vitamin E (mg) | 7.0 | 11.0 |
| Vitamin K (mcg) | 55.0 | 60.0 |
| Calcium (mg) | 1000.0 | 1300.0 |
| Iron (mg) | 10.0 | 8.0 |
| Magnesium (mg) | 130.0 | 240.0 |
| Phosphorus (mg) | 500.0 | 1250.0 |
| Selenium (mcg) | 30.0 | 40.0 |
| Zinc (mg) | 5.0 | 8.0 |
Factors Influencing Intake
A number of factors can influence children’s eating habits and attitudes toward food. Family environment, societal trends, taste preferences, and messages in the media all impact the emotions that children develop in relation to their diet. Television commercials can entice children to consume sugary products, fatty fast foods, excess kcal, refined ingredients, and sodium. Therefore, it is critical that parents and caregivers direct children toward healthy choices.
One way to encourage children to eat healthy foods is to make meals and snacks fun and interesting. Parents should include children in food planning and preparation, for example selecting items while grocery shopping or helping to prepare part of a meal, such as making a salad. At this time, parents can also educate children about kitchen safety. It might be helpful to cut sandwiches, meats, or pancakes into small or interesting shapes. In addition, parents should offer nutritious desserts, such as fresh fruits, instead of calorie-laden cookies, cakes, salty snacks, and ice cream. Additionally, research has found that regularly eating dinner as a family is associated with greater consumption of fruits, vegetables, and less saturated and trans fat.27
18.6 Adolescence
The onset of puberty is the beginning of adolescence and is the bridge between the childhood years and young adulthood. According to the DRI recommendations, adolescence is divided into two age groups: 9 through 13 years, and 14 through 18 years. Some of the important physiological changes that take place during this stage include the development of the primary sex characteristics (the reproductive organs), along with the onset of menstruation in females. This life stage is also characterized by the appearance of secondary sex characteristics, such as the growth of facial and body hair, the development of breasts in girls, the deepening of the voice in boys, and alterations in body proportions. All of these changes, as well as the accompanying mental and emotional adjustments, should be supported with sound nutrition.
The Onset of Puberty (Ages 9 through 13 years)
This period of physical development is divided into two phases. The first phase involves height increases from 20-25%. Puberty is second to the prenatal period in terms of rapid growth as the long bones stretch to their final, adult size. Girls typically grow 2 to 8 inches taller, while boys grow 4 to 12 inches taller. The second phase involves weight gain related to the development of bone, muscle, and fat tissue.
Energy and Macronutrients
 The energy requirements for preteens differ according to biological sex, growth, and activity level. For ages 9 to 13, girls should consume about 1,400-2,200 kcal per day and boys should consume 1,600-2,600 kcal per day. Physically active preteens who regularly participate in sports or exercise need to eat a greater number of kcal to account for increased energy expenditures.
The energy requirements for preteens differ according to biological sex, growth, and activity level. For ages 9 to 13, girls should consume about 1,400-2,200 kcal per day and boys should consume 1,600-2,600 kcal per day. Physically active preteens who regularly participate in sports or exercise need to eat a greater number of kcal to account for increased energy expenditures.
The AMDR recommendations remain 45-65% of total kcal from carbohydrates, 10-30% from protein, and 25-35% from fat. Foods that are high in fiber should make up the bulk of carbohydrate intake.
Micronutrients
Key vitamins needed during puberty include vitamins B12, D, and K. Adequate calcium intake is essential for building bone and preventing osteoporosis later in life. Young females need more iron beginning at the onset of menstruation, while young males need additional iron for the development of lean body mass. Almost all of these needs should be met with dietary choices, not supplements (although iron may be an exception). See Table 18.6.1 for specific recommended micronutrients amounts.
Late Adolescence (Ages 14 through 18 years)
After puberty, the rate of physical growth slows down. Girls stop growing taller around age 16, while boys continue to grow until ages 18-20. One of the psychological and emotional changes that takes place during this life stage includes the desire for independence as adolescents develop individual identities apart from their families. As teenagers make more and more of their own dietary decisions, parents or other caregivers and authority figures should guide them toward appropriate, nutritious choices. One way that teenagers assert their independence is by choosing what to eat. They often have their own money to purchase food and tend to eat more meals away from home. Older adolescents also can be curious and open to new ideas, which includes trying new kinds of food and experimenting with their diet. For example, teens will sometimes skip a main meal and snack instead. That is not necessarily problematic. Their choice of food is more important than the time or place.
 However, too many poor choices can make young people nutritionally vulnerable. Teens should be discouraged from eating fast food, which has a high fat, sugar, and sodium content, or frequenting convenience stores and using vending machines, which typically offer poor nutritional selections. Other challenges that teens may face include obesity and eating disorders. At this life stage, young people still need guidance from parents and other caregivers about nutrition-related matters. It can be helpful to explain to young people how healthy eating habits can support activities they enjoy, such as skateboarding or dancing, or connect to their desires or interests, such as athletic performance or improved cognition.
However, too many poor choices can make young people nutritionally vulnerable. Teens should be discouraged from eating fast food, which has a high fat, sugar, and sodium content, or frequenting convenience stores and using vending machines, which typically offer poor nutritional selections. Other challenges that teens may face include obesity and eating disorders. At this life stage, young people still need guidance from parents and other caregivers about nutrition-related matters. It can be helpful to explain to young people how healthy eating habits can support activities they enjoy, such as skateboarding or dancing, or connect to their desires or interests, such as athletic performance or improved cognition.
As during puberty, growth and development during adolescence differs in males and females. Teenage girls experience a significant increase in body fat, while teenage boys often experience an increase in fat-free and skeletal mass, and a decrease in body fat.28 For both males and females, primary and secondary sex characteristics have fully developed and the rate of growth slows with the end of puberty.
Energy and Macronutrients
Adolescents have increased appetites due to increased nutritional requirements. Nutrient needs are greater in adolescence than at any other time in the life cycle, except during pregnancy. The energy requirements for ages 14 to 18 are 1,800-2,400 kcal for girls and 2,000-3,200 kcal for boys, depending on activity level. The extra energy required for physical development during the teenage years should be obtained from foods that provide nutrients instead of “empty calories.” Also, teens who participate in athletics must make sure to meet their increased energy needs.
Older adolescents are more responsible for their dietary choices than younger children, but parents and caregivers must make sure that teens continue to meet their nutrient needs. The AMDR for carbohydrates remains 45-65% of daily kcal and the adequate intake (AI) of fiber is 25-34 g per day (depending on daily kcal intake). Adolescents require more servings of grain than younger children, and should eat whole grains, such as wheat, oats, barley, and brown rice. The NAM recommends higher intakes of protein for growth in the adolescent population. The AMDR for protein remains 10-30% of daily kcal and lean proteins, such as meat, poultry, fish, beans, nuts, and seeds are excellent ways to meet those nutritional needs. The AMDR for fat remains 25-35% of daily kcal. It is also essential for young athletes and other physically active teens to intake enough fluids, because they are at a higher risk for becoming dehydrated.
Micronutrients
Micronutrient recommendations for adolescents are mostly the same as for adults, though children this age need more of certain minerals to promote bone growth (e.g., calcium and phosphorus, along with iron and zinc for girls). Again, vitamins and minerals should be obtained from food first, with supplementation for certain micronutrients only (such as iron).
The most important micronutrients for adolescents are calcium, vitamin D, vitamin A, and iron. Adequate calcium and vitamin D are essential for building bone mass. The recommendation for calcium is 1,300 mg for both boys and girls. Low-fat milk and cheeses are excellent sources of calcium and help young people avoid saturated fat and cholesterol. It can also be helpful for adolescents to consume products fortified with calcium, such as breakfast cereals and orange juice. Iron supports the growth of muscle and lean body mass. Adolescent girls also need to ensure sufficient iron intake as they start to menstruate. Girls ages 12 to 18 require 15 mg of iron per day. Increased amounts of vitamin C from orange juice and other sources can aid in iron absorption. Also, adequate fruit and vegetable intake allows for meeting vitamin A needs.
Table 18.6.1 Recommended Micronutrient Intakes during Adolescence
| Nutrient | Females, 14-18 Years | Males, 14-18 Years |
| Vitamin A (mcg) | 700.0 | 900.0 |
| Thiamin (mg) | 1.0 | 1.2 |
| Riboflavin (mg) | 1.0 | 1.3 |
| Niacin (mg) | 14 | 16 |
| Vitamin B6 (mg) | 1.2 | 1.3 |
| Folate (mcg) | 400.0 | 300.0 |
| Vitamin B12 (mcg) | 2.4 | 2.4 |
| Vitamin C (mg) | 65.0 | 75.0 |
| Vitamin D (mcg) | 15.0 | 15.0 |
| Vitamin E (mg) | 15.0 | 15.0 |
| Vitamin K (mcg) | 75.0 | 75.0 |
| Calcium (mg) | 1300.0 | 1300.0 |
| Iron (mg) | 15.0 | 11.0 |
| Magnesium (mg) | 360.0 | 410.0 |
| Phosphorus (mg) | 1250.0 | 1250.0 |
| Selenium (mcg) | 55.0 | 55.0 |
| Zinc (mg) | 9.0 | 11.0 |
18.7 Adulthood
Adulthood begins at the end of adolescence and continues until the end of one’s life.
Young Adulthood
Young adulthood is the period from ages 19 to 30 years. It is a stable time compared to childhood and adolescence. Physical growth has been completed and all of the organs and body systems are fully developed. Typically, a young adult who is active has reached his or her physical peak and is in prime health. During this life stage, it is important to continue to practice good nutrition. Healthy eating habits promote metabolic functioning, assist repair and regeneration, and prevent the development of chronic conditions. Proper nutrition and adequate physical activity at this stage not only promote wellness in the present, but also provide a solid foundation for the future.
With the onset of adulthood, good nutrition can help young adults enjoy an active lifestyle. The body of an adult does not need to devote its energy and resources to support the rapid growth and development that characterizes youth. However, the choices made during those formative years can have a lasting impact. Eating habits and preferences developed during childhood and adolescence influence health and fitness into adulthood. Some adults have gotten a healthy start and have established a sound diet and regular activity program, which helps them remain in good condition from young adulthood into their later years. Others carry childhood obesity into adulthood, which adversely affects their health. However, it is not too late to change course and develop healthier habits and lifestyle choices. Therefore, adults must monitor their dietary decisions and make sure their caloric intake provides the energy that they require, without going into excess.
Energy and Macronutrients
Young men typically have higher nutrient needs than young women. For ages 19-30, the energy requirements for women are 1,800-2,400 kcal, and 2,400-3,000 kcal for men, depending on activity level. These estimates do not include women who are pregnant or breastfeeding, who require a higher energy intake. For carbohydrates, the AMDR continues to be 45-65% of daily kcal. All adults, young and old, should eat fewer energy dense carbohydrates, especially refined, sugar dense sources, particularly for those who lead a more sedentary lifestyle. The AMDR for protein is 10-35% of total daily kcal, and should include a variety of lean meat and poultry, eggs, beans, peas, nuts, and seeds. The guidelines also recommend that adults eat at least two 4 oz servings of seafood per week.
It is also important to replace foods that are high in saturated fat with ones that are lower in solid fats and kcal. All adults should limit total fat to 20-35% of their daily kcal and keep saturated fatty acids to less than 10% of total kcal by replacing them with monounsaturated and polyunsaturated fatty acids. The adequate intake for fiber is 22-28 g per day for women and 28-34 g per day for men. Soluble fiber may help improve cholesterol and blood sugar levels, while insoluble fiber can help prevent constipation.
Micronutrients
Micronutrient needs in adults differ slightly according to sex. Young men and women who are very athletic and perspire a great deal may require extra sodium, potassium, and magnesium. Males require more of vitamins A, C, and K along with thiamin, riboflavin, and niacin. Females require extra iron due to menstruation. Therefore, it can be beneficial for some young adults to follow a daily multivitamin regimen to help meet nutrient needs. But as always, it is important to remember “food first, supplements second.”
Table 18.7.1 Recommended Micronutrient Intakes during Adulthood
| Nutrient | Females, 19+ Years | Males, 19+ Years |
| Vitamin A (mcg) | 700.0 | 900.0 |
| Thiamin (mg) | 1.1 | 1.2 |
| Riboflavin (mg) | 1.1 | 1.3 |
| Niacin (mg) | 14.0 | 16.0 |
| Vitamin B6 (mg) | 1.3 (19-50 yr) | 1.3 (19-50 yr) |
| 1.5 (51+ yr) | 1.7 (51+ yr) | |
| Folate (mcg) | 400.0 | 400.0 |
| Vitamin B12 (mcg) | 2.4 | 2.4 |
| Vitamin C (mg) | 75.0 | 90.0 |
| Vitamin D (mcg) | 15.0 (19-70 yr) | 15.0 (19-70 yr) |
| 20.0 (71+ yr) | 20.0 (71+ yr) | |
| Vitamin E (mg) | 15.0 | 15.0 |
| Vitamin K (mcg) | 90.0 | 120.0 |
| Calcium (mg) | 1000.0 (19-50 yr) | 1000.0 (19-70 yr) |
| 1200.0 (51+yr) | 1200.0 (71+ yr) | |
| Iron (mg) | 18.0 (19-50 yr) | 8.0 |
| 8.0 (51+ yr) | ||
| Magnesium (mg) | 310.0 (19-30 yr) | 400.0 (19-30 yr) |
| 320.0 (31+ yr) | 420.0 (31+ yr) | |
| Phosphorus (mg) | 700.0 | 700.0 |
| Selenium (mcg) | 55.0 | 55.0 |
| Zinc (mg) | 8.0 | 11.0 |
Middle Age
Middle age is defined as the period from age 31 to 50. The early period of this stage is very different from the end. For example, during the early years of middle age, many women experience pregnancy, childbirth, and lactation. In the latter part of this life stage, women face perimenopause, which is a transition period that leads up to menopause, or the end of menstruation. A number of physical changes take place in the middle-aged years, including the loss of bone mass in women due to dropping levels of estrogen during menopause. In both men and women, visual acuity declines, and by age 40 there can be a decreased ability to see objects at a close distance.29 All of these are signs of aging, as the human body begins to change in subtle and not-so-subtle ways. However, a middle aged person can remain vital, healthy, and near his or her physical peak with proper diet and adequate exercise.
During this stage of the human life cycle, adults begin to experience the first outward signs of aging. Wrinkles begin to appear, joints may ache after a highly active day, and body fat accumulates. There is also a loss of muscle tone and elasticity in the connective tissue.29 Many people in this stage may also notice a decline in endurance, the onset of wear-and-tear injuries (such as osteoarthritis), and changes in the digestive system. Wounds and other injuries may also take longer to heal. Body composition changes due to fat deposits in the trunk. To maintain health and wellness during the middle-aged years and beyond, it is important to:
- maintain a healthy body weight
- consume nutrient dense foods
- drink alcohol moderately or not at all
- avoid tobacco products
- engage in moderate aerobic physical activity at least 150 minutes per week
- engage in muscle strengthening activity at least two days per week
Energy and Macronutrients
The energy requirements for ages 31 to 50 are 1,800-2,200 kcal for women and 2,200-3,000 kcal for men, depending on activity level. These estimates do not include women who are pregnant or breastfeeding. Middle-aged adults must rely on healthy food sources to meet these needs. Following the dietary guidelines in the middle-aged years provides adequate but not excessive energy, vitamins, and minerals.
The recommended intake for carbohydrates, protein, fat, fiber, and fluids remain the same from young adulthood into middle age. It is important to avoid putting on excess weight and limiting intake of saturated fats and added sugars to help avoid cardiovascular disease, diabetes, and other chronic conditions.
Micronutrients
There are some differences, however, regarding micronutrients. For men, the recommendation for magnesium increases to 420 mg daily, while middle-aged women should increase their intake of magnesium to 320 mg per day. Other key vitamins needed during the middle-aged years include vitamins B6, B12 and folate to prevent elevation of homocysteine, a byproduct of metabolism that can damage arterial walls and lead to atherosclerosis, a cardiovascular condition.
Preventive/Defensive Nutrition
During the middle-aged years, preventive nutrition can promote wellness and help organ systems to function optimally throughout aging. Preventive nutrition is defined as dietary practices directed toward reducing disease and promoting health and well-being. Healthy eating in general, such as eating unrefined carbohydrates instead of refined carbohydrates and avoiding trans fats and saturated fats, helps to promote wellness. However, there are also some things that people can do to target specific concerns. One example is consuming foods high in antioxidants, such as strawberries, blueberries, and other colorful fruits and vegetables, to reduce risk of cancer. Omega-3 fatty acids can help to prevent coronary artery disease. These crucial nutrients are found in oily fish, including salmon, mackerel, tuna, herring, cod, and halibut. Other beneficial fats that are vital for healthy functioning include monounsaturated fats, which are found in plant oils, avocados, and pecans.
Menopause
In the middle-aged years, women undergo a specific change that has a major effect on their health. They begin the process of menopause, typically in their late 40s or early 50s. The ovaries slowly cease to produce estrogen and progesterone, which results in the end of menstruation. Menopausal symptoms can vary, but often include hot flashes, night sweats, and mood changes. The hormonal changes that occur during menopause can lead to a number of physiological changes as well, including alterations in body composition, such as weight gain in the abdominal area. Bone loss is another common condition related to menopause due to the loss of female reproductive hormones. When one loses a significant amount of bone, they likely have osteoporosis, increasing their risk of fractures, which can affect mobility and the ability to complete everyday tasks.30 See Chapter 15 for more information on osteoporosis.
Recommendations for women experiencing menopause or perimenopause (the stage just prior to the end of the menstruation) include31:
- consuming a variety of whole, nutrient dense foods like vegetables, fruits, whole grains, and lean protein sources such as beans and lentils
- avoiding caffeine, spicy foods, and alcohol to help prevent hot flashes
- eating foods rich in calcium, or taking physician prescribed calcium and vitamin D supplements
- reducing sodium intake
- being physically active at least 30 minutes at moderate intensity most days of the week, include strength training activities, and stretching to improve balance and flexibility and reduce the risk of falls and fractures
- drinking plenty of water
18.8 Older Age
The senior years are the period from age 51 until the end of life. A number of physiological and emotional changes take place during this life stage. For example, many older adults face serious health challenges, such as cancer, heart disease, diabetes, or dementia. Both men and women experience a loss of hormone production, muscle mass and strength, and undergo changes in body composition. Fat deposits build up in the abdominal area, which increases the risk for type 2 diabetes and  cardiovascular disease. The skin becomes thinner and may take longer to heal after an injury. Also in the later years, the heart has to work harder because each pump is not as efficient as it used to be. Kidneys are not as effective in excreting metabolic products such as sodium and potassium, which can alter water balance and increase the risk for dehydration. In addition, immune function decreases and there is lower efficiency in the absorption of vitamins and minerals.
cardiovascular disease. The skin becomes thinner and may take longer to heal after an injury. Also in the later years, the heart has to work harder because each pump is not as efficient as it used to be. Kidneys are not as effective in excreting metabolic products such as sodium and potassium, which can alter water balance and increase the risk for dehydration. In addition, immune function decreases and there is lower efficiency in the absorption of vitamins and minerals.
In addition, disorders of the nervous system can have profound effects. Dementia is the umbrella term for changes in the normal activity of the brain. Elderly adults who suffer from dementia may experience memory loss, agitation, and delusions. More than five million Americans have Alzheimer’s disease, the most common form of dementia. It is the sixth leading cause of death in the US.32 Neurological disorder and psychological conditions, such as depression, can influence attitudes toward food, along with the ability to prepare or ingest food. They might lead some adults to overindulge to compensate for stress or emotions that are difficult to handle. Other adults might eat less or pay less attention to their diet and nutritional needs. Older adults may also need guidance from dietitians and healthcare professionals to make the best dietary choices for this stage of life.
In older age, blood pressure rises and the immune system may have more difficulty battling invaders and infections. The skin becomes more wrinkled and hair has turned gray or white or fallen out, resulting in hair thinning. Older adults may gradually lose an inch or two in height. Also, short-term memory might not be as keen as it once was.
Being either underweight or overweight is a major concern for the elderly. However, many older adults remain in relatively good health and continue to be active into their golden years. Good nutrition is often the key to maintaining health later in life. In addition, the fitness and nutritional choices made earlier in life set the stage for continued health and happiness. Older adults should continue to consume nutrient dense foods and remain physically active. However, deficiencies are more common after age 60, primarily due to reduced intake or absorption. The loss of mobility among frail, home-bound elderly adults also impacts their access to healthy, diverse foods.
Energy and Macronutrients
Due to reductions in lean body mass and metabolic rate, older adults require less energy than younger adults. The energy requirements for people ages 51 and over are 1,600-2,200 kcal for women and 2,000-2,800 kcal for men, depending on activity level. The decrease in physical activity that is typical of older adults also influences nutritional requirements. The AMDRs for carbohydrates, protein, and fat remain the same from middle age into old age. However, it is recommended that the elderly consume 1.2-2.0 g of protein per kg body weight to help prevent significant muscle loss.33 Older adults should choose more unrefined carbohydrates such as whole grains and brown rice instead of refined grains. Fiber is especially important in preventing constipation and diverticulitis, and may also reduce the risk of colon cancer. Protein should be lean and healthy fats, such as omega-3 fatty acids, are part of any good diet.
Micronutrients
An increase in certain micronutrients can help maintain health during this life stage. The recommendations for calcium increase to 1,200 mg per day for women beginning at age 51 and men at age 71 to slow bone loss. Also to help protect bones, vitamin D recommendations increase from 15 to 20 mcg per day for men and women. Vitamin B6 recommendations rise to 1.7 mg per day for older men and 1.5 mg per day for older women to help lower levels of homocysteine and protect against cardiovascular disease. For elderly women, higher iron levels are no longer needed postmenopause and recommendations decrease to 8 mg per day. People over age 50 should eat foods rich with all of these micronutrients.
Nutritional Concerns for Older Adults
Dietary choices can help improve health during this life stage and address some of the nutritional concerns that many older adults face. In addition, there are specific concerns related to nutrition that affect adults in their later years. They include medical problems, such as disability and disease, which can impact diet and activity level. For example, dental problems can lead to difficulties with chewing and swallowing, which in turn can make it hard to maintain a healthy diet. The use of dentures or the preparation of chopped or pureed foods can help solve this problem. There also is a decreased thirst response in the elderly, and the kidneys have a decreased ability to concentrate urine, both of which can lead to dehydration.
Sensory Issues
At about age 60, taste buds begin to decrease in size and number. As a result, the taste threshold is higher in older adults, meaning that more of the same flavor must be present to detect the taste. Many elderly people lose the ability to distinguish between salty, sour, sweet, and bitter flavors. This can make food seem less appealing and decrease the appetite. An intake of foods high in sugar and sodium can increase due to an inability to discern those tastes. The sense of smell also decreases, which impacts attitudes toward food. Sensory issues may also affect the digestion because the taste and smell of food stimulates the secretion of digestive enzymes in the mouth, stomach, and pancreas.
Gastrointestinal Issues
A number of gastrointestinal issues can affect food intake and digestion among the elderly. Saliva production decreases with age, which affects chewing, swallowing, and taste. Other digestive secretions decline later in life as well, which can lead to atrophic gastritis (inflammation of the lining of the stomach). This interferes with the absorption of some vitamins and minerals. Reduction of the digestive enzyme lactase results in a decreased tolerance for dairy products. Slower gastrointestinal motility can result in more constipation, gas, and bloating, and can also be tied to low fluid intake, decreased physical activity, and a diet low in fiber, fruits, and vegetables.
Dysphagia
Some older adults have difficulty getting adequate nutrition because of the disorder dysphagia, which impairs the ability to swallow. Any damage to the parts of the brain that control swallowing can result in dysphagia, therefore having a cerebrovascular accident, more commonly called a stroke, is a common cause. Dysphagia is also associated with advanced dementia because of overall brain function impairment. To assist older adults suffering from dysphagia, it can be helpful to alter food consistency. For example, solid foods can be chopped, ground, or pureed to allow a more successful and safe swallow. This decreases the risk of aspiration, which occurs when food enters the respiratory tract and can result in pneumonia. Typically, speech therapists, physicians, and dietitians work together to determine the appropriate diet for dysphagia patients.
Vision Problems
Many older people suffer from vision problems and a loss of vision. Age-related macular degeneration is the leading cause of blindness in Americans over age 60.34 This disorder can make food planning and preparation extremely difficult and people who suffer from it often must depend on caregivers for their meals. Self-feeding may be difficult if an elderly person cannot see his or her food clearly. Friends and family members can help older adults with shopping and cooking. Food-assistance programs for older adults (such as Meals on Wheels) can also be helpful.
Diet may help to prevent macular degeneration. Consuming colorful fruits and vegetables increases the intake of lutein and zeaxanthin. Several studies have shown that these antioxidants provide protection for the eyes. Lutein and zeaxanthin are found in green, leafy vegetables such as spinach, kale, and collard greens, and also corn, peaches, squash, broccoli, Brussels sprouts, orange juice, and honeydew melon.35
Obesity in Old Age
Similar to other life stages, obesity is a concern for the elderly. Adults over age 60 are more likely to be obese than young or middle-aged adults. As explained previously, excess body weight has severe consequences. Being overweight or obese increases the risk for potentially fatal conditions that can afflict the elderly. They include cardiovascular disease, which is the leading cause of death in the US and type 2 diabetes, the seventh leading cause of death in the US annually.
For older adults who are overweight or obese, dietary changes to promote weight loss should be combined with an exercise program to protect muscle mass. This is because dieting reduces muscle as well as fat, which can exacerbate the loss of muscle mass due to aging. Although weight loss among the elderly can be beneficial, it is best to be cautious and consult with a healthcare professional before beginning a weight loss program.
The Anorexia of Aging
In addition to concerns about obesity among senior citizens, being underweight can be a major problem. A condition known as the anorexia of aging is characterized by poor food intake, which results in dangerous weight loss. This major health problem among the elderly leads to a higher risk for immune deficiency, frequent falls, muscle loss, and cognitive deficits. Reduced muscle mass (sarcopenia) and physical activity mean that older adults need fewer kcal per day to maintain a normal weight. It is important for health care providers to examine the causes for anorexia of aging among their patients, which can vary from one individual to another. Understanding why some elderly people eat less as they age can help healthcare professionals assess the risk factors associated with this condition. Decreased intake may be due to disability or the lack of a motivation to eat. Also, many older adults skip at least one meal each day, sometimes because of financial reasons. As a result, some elderly people are unable to meet even reduced energy needs.
Nutritional interventions should focus primarily on a healthy diet. Remedies can include increasing the frequency of meals and adding healthy, high-calorie foods (such as nuts, potatoes, whole-grain pasta, and avocados) to the diet. Liquid supplements between meals may help to improve caloric intake. Health care professionals should consider a patient’s habits and preferences when developing a nutritional treatment plan. After a plan is in place, patients should be weighed on a weekly basis until they show improvement.
Longevity and Nutrition
The foods you consume in your younger years influence your health as you age. Good nutrition and regular physical activity can help you live longer and healthier. Conversely, poor nutrition and a lack of exercise can shorten your life and lead to medical problems. The right foods provide numerous benefits at every stage of life. They help an infant grow, an adolescent develop mentally and physically, a young adult achieve his or her physical peak, and an older adult cope with aging. Nutritious foods form the foundation of a healthy life at every age.
Key Takeaways
- Starting BMI determines how much weight a woman needs to gain throughout her pregnancy. In an average pregnancy, a woman gains an extra 30 lb.
- During the second and third trimesters, a woman’s energy requirements increase by 340 kcal per day for the second trimester and 450 kcal per day for the third trimester. For the first six months of life, children should consume breast milk exclusively.
- For the next six months, solid foods should be introduced gradually into an infant’s diet as parents and caregivers continue to provide breast milk.
- Breast milk is ideal for infants and provides all of the nutrients they need to grow and develop. Breastfeeding provides numerous benefits for both a mother and her infant.
- By the toddler years, young children are able to self-feed and begin to develop eating habits and preferences.
- Some food- and nutrition-related problems that can occur during the toddler years include choking, picky eating and food jags, early childhood caries, and iron deficiency anemia.
- The recommended intakes of macronutrients and micronutrients for children are higher relative to body size compared with nutrient needs during adulthood. Children’s daily energy needs vary depending on their level of physical activity.
- Beginning in adolescence, some micronutrient needs begin to differ by biological sex.
- Nutritional concerns for middle-aged adults relate to menopause and the prevention of chronic disease.
- Older adults are more susceptible to medical problems, such as disability and disease, which can impact appetite, the ability to plan and prepare food, chewing and swallowing, self-feeding, and general nutrient intake.
Portions of this chapter were taken from OER Sources listed below:
Tharalson, J. (2019). Nutri300:Nutrition. https://med.libretexts.org/Courses/Sacremento_City_College/SSC%3A_Nutri_300_(Tharalson)
Titchenal, A., Calabrese, A., Gibby, C., Revilla, M.K.F., & Meinke, W. (2018). Human Nutrition. University of Hawai'i at Manoa Food Science and Human Nutrition Program Open Textbook. https://pressbooks.oer.hawaii.edu
Additional References:
- Centers for Disease Control and Prevention. (2020, February 26). Before pregnancy. Information for men. https://www.cdc.gov/preconception/men.html
- Jarlenski, M. P., Bennett, W. L., Bleich, S. H., Barry, C. L., & Stuart, E. A. (2014). Effects of breastfeeding on postpartum weight loss among US women. Preventive Medicine, 69, 146-50. https://doi:10.1016/j.ypmed.2014.09.018
- Most, J., Dervis, S., Haman, F., Adamo, K. B., & Redman, L. M. (2019). Energy intake requirements in pregnancy. Nutrients, 11(8), 1812. https://doi:10.3390/nu/11081812
- Office on Women’s Health. (2019, March 14). Staying Healthy and Safe. United States Department of Health and Human Services.https://www.womenshealth.gov/pregnancy/youre-pregnant-now-what/staying-healthy-and-safe/#1
- American College of Obstetricians and Gynecologists. (2010). Moderate caffeine consumption during pregnancy. Committee Opinion No. 462. Obstetrics & Gynecology 116, 467-8. https://www.acog.org/clinical/clinical-guidance/committee-opinion/articles/2010/08/moderate-caffeine-consumption-during-pregnancy
- Centers for Disease Control and Prevention. (2016, December 16). Listeria (listeriosis). https://www.cdc.gov/listeria/risk-groups/pregnant-women.html
- Lumish, R. A., Young, S. L., Lee, S., Cooper, E., Presman, E., Guillet, R., & O’Brien, K. O. (2014). Gestation iron deficiency is associated with pica behavior in adolescents. The Journal of Nutrition, 144(10), 1533-1539. doi:10.3945/jn.114.192070.
- Zhou, T., Sun, D., Li, X., Heianza, Y., Nisa, H., Hu, G., Pei, X., Shang, X., & Qi, L. (2018). Prevalence and trends in gestational diabetes mellitus among women in the United States, 2006-2016. Diabetes, 67(Suppl1). https://doi:10.2237/db18-121-OR
- American Pregnancy Association. (n.d.). Breastfeeding vs bottle feeding formula. https://americanpregnancy.org/breastfeeding/breastfeeding-vs-bottle-feeding-formula/
- Centers for Disease Control and Prevention. (2019, December 31). Breastfeeding report card, United States 2018. https://www.cdc.gov/breastfeeding/data/reportcard.htm
- World Health Organization (2020. April 1). Infant and young children feeding: Key facts. https://www.who.int/news-room/fact-sheets/detail/infant-and-young-child-feeding
- United States Department of Health and Human Services. (2011, January 20). Executive summary: The Surgeon General’s call to action to support breastfeeding. Office of the Surgeon General. https://www.hhs.gov/sites/default/files/breastfeeding-call-to-action-executive-summary.pdf
- Pillay, J., & Davis, T. J. (2020, April 27). Physiology, lactation. StatPearls. https://www.ncbi.nlm.nih.gov/books/NBK499981/
- Ballard, O., & Morrow, A. L. (2013). Human milk composition: Nutrients and bioactive factors. Pediatric Clinics of North America, 60(1), 49-74. https://doi:10.1016.j.pcl.2012.10.002
- American Pregnancy Association. (2020, June, 25). Breastfeeding: Overview. http://www.americanpregnancy.org/firstyearoflife/breastfeedingoverview.htm.
- Centers for Disease Control and Prevention. (2019, December 28). Alcohol. https://www.cdc.gov/breastfeeding/breastfeeding-special-circumstances/vaccinations-medications-drugs/alcohol.html
- Bravi, F., Wiens, F., Decarli, A., Dal Pont, A., Agostoni, C., & Ferraroni, M. (2016). Impact of maternal nutrition on breast-milk composition: a systematic review. The American Journal of Clinical Nutrition, 104(3), 646-662. https://doi:10.3945/ajcn.115.120881.
- McMillan, B. (2008). Illustrated atlas of the human body. Weldon Owen.
- Centers for Disease Control and Prevention. (2019, December 19). Vitamin K deficiency bleeding. https://www.cdc.gov/ncbddd/vitamink/faqs.html
- Centers for Disease Control and Prevention. (2019, October 17). When, what, and how to introduce solid foods. https://www.cdc.gov/nutrition/infantandtoddlernutrition/foods-and-drinks/when-to-introduce-solid-foods.html
- United States Department of Agriculture. (2016, October). Healthy eating for preschoolers. ChooseMyPlate. https://choosemyplate-prod.azureedge.net/sites/default/files/tentips/healthy_eating_for_preschoolers.pdf)
- The Ellyn Satter Institute. (n.d.). Division of responsibility in feeding. https://www.ellynsatterinstitute.org/how-to-feed/the-division-of-responsibility-in-feeding/
- World Health Organization. (2019, September 3). Facts and figures on childhood obesity. https://www.who.int/end-childhood-obesity/facts/en/
- Fryar, C. D., Carroll, M. D., & Ogden, C. L. (2014). Prevalence of overweight and obesity among children and adolescents: United States, 1963-1965 through 2011-2012. National Center for Health Statistics. https://www.cdc.gov/nchs/data/hestat/obesity_child_11_12/obesity_child_11_12.pdf
- Hales, C. M., Carroll, M. D., Fryar, C. D., & Ogden, C. L. (2017). Prevalence of obesity among adults and youth: 2015-2016. National Center for Health Statistics. Data Brief, no 288. https://www.cdc.gov/nchs/products/databriefs/db288.htm
- Ervin, R. B., Kit, B. K., Carroll, M. D., & Ogden, C. L. (2012, February). Consumption of added sugar among US Children and Adolescents, 2005-2008. National Center for Health Statistics. Data Brief, no. 87. https://www.cdc.gov/nchs/products/databriefs/db87.htm
- Gillman, M. W., Rifas-Shiman, S. L., Frazier, L., Rockett, H. R., Camargo, C. A., Field, A. E., Berkey, C. S., & Colditz, G. A. (2000). Family dinner and diet quality among older children and adolescents. Archives of Family Medicine 9, 235-240.
- Loomba-Albrecht, L.A., & Styne, D. M. (2009). Effect of puberty on body composition. Current Opinion in Endocrinology, Diabetes and Obesity, 16(1), 10-15. https://doi:10.3945/ajcn.115.120881
- Poland, E.U., & Taylor, D.R. (2003). Journey across the lifespan: Human development and health promotion. Davis Company.
- National Osteoporosis Foundation. (n.d.). What is osteoporosis and what causes it? https://www.nof.org/patients/what-is-osteoporosis/
- Wolfram, T. (2019). Eating right during menopause. Academy of Nutrition and Dietetics. https://www.eatright.org/health/wellness/healthy-aging/eating-right-during-menopause
- Alzheimer’s Association. (n.d.). Facts and Figures. https://www.alz.org/alzheimers-dementia/facts-figures
- Baum, J.I.,Kim, I-Y., & Wolfe, R.R. (2016). Protein consumption and the elderly. Nutrients, 8(6), 359. doi:10.3390%2Fnu8060359
- National Eye Institute. (2019. July 17). Age-related macular degeneration (AMD) data and statistics. National Institutes of Health. https://www.nei.nih.gov/learn-about-eye-health/resources-for-health-educators/eye-health-data-and-statistics/age-related-macular-degeneration-amd-data-and-statistics
- Eisenhauer, B., Natoli, S., Liew, G., & Flood, V. M. (2017). Lutein and zeaxanthin-food sources, bioavailability and dietary variety in age-related macular degeneration protection. Nutrients, 9(2), 120. https://doi.org/10.3390/nu9020120
Scientific exploration of how an organism nourishes itself and how this nourishment affects personal, population, and planetary health.
any abnormal condition affecting the health of organisms, characterized by specific signs and symptoms
Is a process of heating a food or beverage to eliminate pathogens and extend shelf life.
things that cannot be easily seen and are usually reported by a patient such as headache, dizziness, pain, or nausea
Table 1: Recommended Dietary Allowances (RDA) and Adequate Intakes (AIs) for Water Soluble Vitamins
| Age (yr) | Thiamin (mg)
RDA |
Riboflavin (mg) RDA | Niacin (mg) RDA | Pantothenic acid (mg) AI | Vitamin B6 (mg) RDA | Biotin (mcg) | Folate (mcg) RDA | Vitamin B12 (mcg) RDA | Vitamin C (mg) RDA |
| Infants | |||||||||
| 0-0.5 | 0.2 | 0.3 | 2 | 1.7 | 0.1 | 5 | 65 | 0.4 | 40 |
| 0.5-1 | 0.3 | 0.4 | 4 | 1.8 | 0.3 | 6 | 80 | 0.5 | 50 |
| Children | |||||||||
| 1-3 | 0.5 | 0.5 | 6 | 2 | 0.5 | 8 | 150 | 0.9 | 15 |
| 4-8 | 0.6 | 0.6 | 8 | 3 | 0.6 | 12 | 200 | 1.2 | 25 |
| 9-13 | 0.9 | 0.9 | 12 | 4 | 1.0 | 20 | 300 | 1.8 | 45 |
| Males | |||||||||
| 14-18 | 1.2 | 1.3 | 16 | 5 | 1.3 | 25 | 400 | 2.4 | 75 |
| 19-30 | 1.2 | 1.3 | 16 | 5 | 1.3 | 30 | 400 | 2.4 | 90 |
| 31-50 | 1.2 | 1.3 | 16 | 5 | 1.3 | 30 | 400 | 2.4 | 90 |
| 51-70 | 1.2 | 1.3 | 16 | 5 | 1.7 | 30 | 400 | 2.4 | 90 |
| > 70 | 1.2 | 1.3 | 16 | 5 | 1.7 | 30 | 400 | 2.4 | 90 |
| Females | |||||||||
| 14-18 | 1.0 | 1.0 | 14 | 5 | 1.2 | 25 | 400 | 2.4 | 65 |
| 19-30 | 1.1 | 1.1 | 14 | 5 | 1.3 | 30 | 400 | 2.4 | 75 |
| 31-50 | 1.1 | 1.1 | 14 | 5 | 1.3 | 30 | 400 | 2.4 | 75 |
| 51-70 | 1.1 | 1.1 | 14 | 5 | 1.5 | 30 | 400 | 2.4 | 75 |
| > 70 | 1.1 | 1.1 | 14 | 5 | 1.5 | 30 | 400 | 2.4 | 75 |
| Pregnancy | |||||||||
| ≤ 18 | 1.4 | 1.4 | 18 | 6 | 1.9 | 30 | 600 | 2.6 | 80 |
| 19-30 | 1.4 | 1.4 | 18 | 6 | 1.9 | 30 | 600 | 2.6 | 85 |
| 31-50 | 1.4 | 1.4 | 18 | 6 | 1.9 | 30 | 600 | 2.6 | 85 |
| Lactation | |||||||||
| ≤ 18 | 1.4 | 1.6 | 17 | 7 | 1.9 | 35 | 500 | 2.8 | 115 |
| 19-30 | 1.4 | 1.6 | 17 | 7 | 1.9 | 35 | 500 | 2.8 | 120 |
| 31-50 | 1.4 | 1.6 | 17 | 7 | 1.9 | 35 | 500 | 2.8 | 120 |
Table 2: Recommended Dietary Allowances (RDA) and Adequate Intakes (AIs) for Fat Soluble Vitamins and Choline
| Age (yr) | Vitamin A (mg) RDA | Vitamin D (mcg) RDA | Vitamin E (mg) RDA | Vitamin K (mcg) AI | Choline (mg) AI |
| Infants | |||||
| 0-0.5 | 400 | 10 | 4 | 2 | 125 |
| 0.5-1 | 500 | 10 | 5 | 2.5 | 150 |
| Children | |||||
| 1-3 | 300 | 15 | 6 | 30 | 200 |
| 4-8 | 400 | 15 | 7 | 55 | 250 |
| 9-13 | 600 | 15 | 11 | 60 | 375 |
| Males | |||||
| 14-18 | 900 | 15 | 15 | 75 | 550 |
| 19-30 | 900 | 15 | 15 | 120 | 550 |
| 31-50 | 900 | 15 | 15 | 120 | 550 |
| 51-70 | 900 | 15 | 15 | 120 | 550 |
| > 70 | 900 | 20 | 15 | 120 | 550 |
| Females | |||||
| 14-18 | 700 | 15 | 15 | 75 | 400 |
| 19-30 | 700 | 15 | 15 | 90 | 425 |
| 31-50 | 700 | 15 | 15 | 90 | 425 |
| 51-70 | 700 | 15 | 15 | 90 | 425 |
| > 70 | 700 | 20 | 15 | 790 | 425 |
| Pregnancy | |||||
| ≤ 18 | 750 | 15 | 15 | 75 | 450 |
| 19-30 | 770 | 15 | 15 | 90 | 450 |
| 31-50 | 770 | 15 | 15 | 90 | 450 |
| Lactation | |||||
| ≤ 18 | 1,200 | 15 | 19 | 75 | 550 |
| 19-30 | 1,300 | 15 | 19 | 90 | 550 |
| 31-50 | 1,300 | 15 | 19 | 90 | 550 |
Table 3: Tolerable Upper Limits (UL) for Vitamins
| Age (yr) | Niacin (mg) | Vitamin B6 (mg) | Folate (mcg) | Vitamin C (mg) | Vitamin A (mg) | Vitamin D (mcg) | Vitamin E (mg) | Choline (mg) |
| Infants | ||||||||
| 0-0.5 | ― | ― | ― | ― | 600 | 25 | ― | ― |
| 0.5-1 | ― | ― | ― | ― | 600 | 38 | ― | ― |
| Children | ||||||||
| 1-3 | 10 | 30 | 300 | 400 | 600 | 63 | 200 | 1,000 |
| 4-8 | 15 | 40 | 400 | 650 | 900 | 75 | 300 | 1,000 |
| Adolescents | ||||||||
| 9-13 | 20 | 60 | 600 | 1,200 | 1,700 | 100 | 600 | 2,000 |
| 14-18 | 30 | 80 | 800 | 1,800 | 2,800 | 100 | 800 | 3,000 |
| Adults | ||||||||
| 19-70 | 35 | 100 | 1,000 | 2,000 | 3,000 | 100 | 1,000 | 3,500 |
| > 70 | 35 | 100 | 1,000 | 2,000 | 3,000 | 100 | 1,000 | 3,500 |
| Pregnancy | ||||||||
| ≤ 18 | 35 | 80 | 800 | 1,800 | 2,800 | 100 | 800 | 3,000 |
| 19-50 | 35 | 100 | 1,000 | 2,000 | 3,000 | 100 | 1,000 | 3,500 |
| Lactation | ||||||||
| ≤ 18 | 30 | 80 | 800 | 1,800 | 2,800 | 100 | 800 | 3,000 |
| 19-50 | 35 | 100 | 1,000 | 2,000 | 3,000 | 100 | 1,000 | 3,500 |
Table 4: Recommended Dietary Allowances (RDA) and Adequate Intakes (AIs) for Major Minerals
| Age (yr) | Sodium (mg) AI | Chloride (mg) AI | Potassium (mg) AI | Calcium (mg) RDA | Phosphorus (mg) RDA | Magnesium (mg) RDA |
| Infants | ||||||
| 0-0.5 | 120 | 180 | 400 | 200 | 100 | 30 |
| 0.5-1 | 370 | 570 | 700 | 260 | 275 | 75 |
| Children | ||||||
| 1-3 | 1,000 | 1,500 | 3,000 | 700 | 460 | 80 |
| 4-8 | 1,200 | 1,900 | 3,800 | 1,000 | 500 | 130 |
| Males | ||||||
| 9-13 | 1,500 | 2,300 | 4,500 | 1,300 | 1,250 | 240 |
| 14-18 | 1,500 | 2,300 | 4,700 | 1,300 | 1,250 | 410 |
| 19-30 | 1,500 | 2,300 | 4,700 | 1,000 | 700 | 400 |
| 31-50 | 1,500 | 2,300 | 4,700 | 1,000 | 700 | 420 |
| 51-70 | 1,300 | 2,000 | 4,700 | 1,000 | 700 | 420 |
| > 70 | 1,200 | 1,800 | 4700 | 1,200 | 700 | 420 |
| Females | ||||||
| 9-13 | 1,500 | 2,300 | 4,500 | 1,300 | 1,250 | 240 |
| 14-18 | 1,500 | 2,300 | 4,700 | 1,300 | 1,250 | 360 |
| 19-30 | 1,500 | 2,300 | 4,700 | 1,000 | 700 | 310 |
| 31-50 | 1,500 | 2,300 | 4,700 | 1,000 | 700 | 320 |
| 51-70 | 1,300 | 2,000 | 4,700 | 1,200 | 700 | 320 |
| > 70 | 1,200 | 1,800 | 4,700 | 1,200 | 700 | 320 |
| Pregnancy | ||||||
| ≤ 18 | 1,500 | 2,300 | 4,700 | 1,300 | 1,250 | 400 |
| 19-30 | 1,500 | 2,300 | 4,700 | 1,000 | 700 | 350 |
| 31-50 | 1,500 | 2,300 | 4,700 | 1,000 | 700 | 360 |
| Lactation | ||||||
| ≤ 18 | 1,500 | 2,300 | 5,100 | 1,300 | 1,250 | 360 |
| 19-30 | 1,500 | 2,300 | 5,100 | 1,000 | 700 | 310 |
| 31-50 | 1,500 | 2,300 | 5,100 | 1,000 | 700 | 320 |
Table 5: Tolerable Upper Limits (UL) for Major Minerals
| Age (yr) | Sodium (mg) | Chloride (mg) | Calcium (mg) | Phosphorus (mg) | Magnesium (mg) |
| Infants | |||||
| 0-0.5 | ― | ― | 1,000 | ― | ― |
| 0.5-1 | ― | ― | 1,500 | ― | ― |
| Children | |||||
| 1-3 | 1,500 | 2,300 | 2,500 | 3,000 | 65 |
| 4-8 | 1,900 | 2,900 | 2,500 | 3,000 | 110 |
| Adolescents | |||||
| 9-13 | 2,200 | 3,400 | 3,000 | 4,000 | 350 |
| 14-18 | 2,300 | 3,600 | 3,000 | 4,000 | 350 |
| Adults | |||||
| 19-70 | 2,300 | 3,600 | 2,000-2,500 | 4,000 | 350 |
| > 70 | 2,300 | 3,600 | 2,000 | 3,000 | 350 |
| Pregnancy | |||||
| ≤ 18 | 2,300 | 3,600 | 3,000 | 3,500 | 350 |
| 19-50 | 2,300 | 3,600 | 2,500 | 3,500 | 350 |
| Lactation | |||||
| ≤ 18 | 2,300 | 3,600 | 3,000 | 4,000 | 350 |
| 19-50 | 2,300 | 3,600 | 2,500 | 4,000 | 350 |
Table 6: Recommended Dietary Allowances (RDA) and Adequate Intakes (AIs) for Trace Minerals
| Age (yr) | Iron (mg) RDA | Zinc (mg) RDA | Iodine (mcg) RDA | Copper (mg) RDA | Selenium (mcg) RDA | Chromium (mcg) AI | Manganese (mg) AI | Molybdenum (mcg) RDA | Fluoride (mg) AI |
| Infants | |||||||||
| 0-0.5 | 0.27 | 2 | 110 | 200 | 15 | 0.2 | 0.003 | 2 | 0.01 |
| 0.5-1 | 11 | 3 | 130 | 220 | 20 | 5.5 | 0.6 | 3 | 0.5 |
| Children | |||||||||
| 1-3 | 7 | 3 | 90 | 340 | 20 | 11 | 1.2 | 17 | 0.7 |
| 4-8 | 10 | 5 | 90 | 440 | 30 | 15 | 1.5 | 22 | 1 |
| Males | |||||||||
| 9-13 | 8 | 8 | 120 | 700 | 40 | 25 | 1.9 | 34 | 2 |
| 14-18 | 11 | 11 | 150 | 890 | 55 | 35 | 2.2 | 43 | 3 |
| 19-30 | 8 | 11 | 150 | 900 | 55 | 35 | 2.3 | 45 | 4 |
| 31-50 | 8 | 11 | 150 | 900 | 55 | 35 | 2.3 | 45 | 4 |
| 51-70 | 8 | 11 | 150 | 900 | 55 | 30 | 2.3 | 45 | 4 |
| > 70 | 8 | 11 | 150 | 900 | 55 | 30 | 2.3 | 45 | 4 |
| Females | |||||||||
| 9-13 | 8 | 8 | 120 | 700 | 50 | 21 | 1.6 | 34 | 2 |
| 14-18 | 15 | 9 | 150 | 890 | 55 | 24 | 1.6 | 43 | 3 |
| 19-30 | 18 | 8 | 150 | 900 | 55 | 25 | 1.8 | 45 | 3 |
| 31-50 | 18 | 8 | 150 | 900 | 55 | 25 | 1.8 | 45 | 3 |
| 51-70 | 8 | 8 | 150 | 900 | 55 | 20 | 1.8 | 45 | 3 |
| > 70 | 8 | 8 | 150 | 900 | 55 | 20 | 1.8 | 45 | 3 |
| Pregnancy | |||||||||
| ≤ 18 | 27 | 12 | 220 | 1,000 | 60 | 29 | 2.0 | 50 | 3 |
| 19-30 | 27 | 11 | 220 | 1,000 | 60 | 30 | 2.0 | 50 | 3 |
| 31-50 | 27 | 11 | 220 | 1,000 | 60 | 30 | 2.0 | 50 | 3 |
| Lactation | |||||||||
| ≤ 18 | 10 | 13 | 290 | 1,300 | 70 | 44 | 2.6 | 50 | 3 |
| 19-30 | 9 | 12 | 290 | 1,300 | 70 | 45 | 2.6 | 50 | 3 |
| 31-50 | 9 | 12 | 290 | 1,300 | 70 | 45 | 2.6 | 50 | 3 |
Table 7: Tolerable Upper Limits (UL) for Trace Minerals
| Age (yr) | Iron (mg) | Zinc (mg) | Iodine (mcg) | Copper (mg) | Selenium (mcg) | Manganese (mg) | Molybdenum (mcg) | Fluoride (mg) |
| Infants | ||||||||
| 0-0.5 | 40 | 4 | ― | ― | 45 | ― | ― | 0.7 |
| 0.5-1 | 40 | 5 | ― | ― | 60 | ― | ― | 0.9 |
| Children | ||||||||
| 1-3 | 40 | 7 | 200 | 1,000 | 90 | 2 | 300 | 1.3 |
| 4-8 | 40 | 12 | 300 | 3,000 | 150 | 3 | 600 | 2.2 |
| Adolescents | ||||||||
| 9-13 | 40 | 23 | 600 | 5,00 | 280 | 6 | 1,100 | 10 |
| 14-18 | 45 | 24 | 900 | 8,00 | 400 | 9 | 1,700 | 10 |
| Adults | ||||||||
| 19-70 | 45 | 40 | 1,100 | 10,000 | 400 | 11 | 2,000 | 10 |
| > 70 | 45 | 40 | 1,100 | 10,000 | 400 | 11 | 2,000 | 10 |
| Pregnancy | ||||||||
| ≤ 18 | 45 | 34 | 900 | 8,000 | 400 | 9 | 1,700 | 10 |
| 19-50 | 45 | 40 | 1,100 | 10,000 | 400 | 11 | 2,000 | 10 |
| Lactation | ||||||||
| ≤ 18 | 45 | 34 | 900 | 8,000 | 400 | 9 | 1,700 | 10 |
| 19-50 | 45 | 40 | 1,100 | 10,000 | 400 | 11 | 2,000 | 10 |
Table 8: Acceptable Macronutrient Distribution Ranges (AMDR)
| Macronutrient | Children, 1-3 years | Children, 4-18 years | Adults, 19+ years |
| Carbohydrate | 45-65% | 45-65% | 45-65% |
| Fiber | 19 g/d | 25-38 g/d | 25-38 g/d |
| Added Sugar | ≤ | ≤ | ≤ 25% |
| Protein | 5-20% | 10-30% | 10-35% |
| Fat | 30-40% | 25-35% | 20-35% |
| Saturated Fat | <10% | <10% | <10% |
| Omega-6 | 5-10% | 5-10% | 5-10% |
| Omega 3 | 0.6-12% | 0.6-12% | 0.6-12% |
Source: Adapted from the Dietary Reference Intakes series, National Academies Press. Copyright 1997, 1998, 2000, 2001, 2002, 2004, 2005, 2011, and 2013 by the National Academy of Sciences.
In nutrition there are two systems of commonly used measurements: Metric and US Customary. We need both because the US hasn't yet adopted the metric system completely.
These are commonly used prefixes for the Metric System
| Micro- (u or mc) | 1/1,000,000 (one millionth) |
| Milli- (m) | 1/1000 (one thousandth) |
| Centi- (c) | 1/100 (one hundredth) |
| Deci- (d) | 1/10 (one tenth) |
| Kilo- (k) | 1000x (one thousand times) |
Measures of Mass
| Metric System | US Customary System | Conversions |
| Microgram (ug or mcg) | ounce (oz) | 1 oz = 28.35 g |
| Milligram (mg) | pound (lb) | 1 lb = 16 oz |
| Gram (g) | 1 lb = 454 g | |
| Kilogram (kg) | 1 kg = 2.205 lbs |
Measures of Volume
| Metric System | US Customary System | Conversions |
| Milliliter (mL) | Teaspoon (t. or tsp) | 1 tsp = 5 mL |
| Deciliter (dL) | Tablespoon (T. or tbsp) | 1 T. = 3 tsp = 15 mL |
| Liter (L) | Fluid ounce (fl oz) | 1 fl oz = 2 T. = 30 mL |
| Cup (c) | 1 c = 8 fl oz = 237 mL | |
| Pint (pt) | 1 pt = 2 c = 16 fl oz | |
| Quart (qt) | 1 qt = 4 c = 32 fl oz = 0.95 L | |
| Gallon (gal) | 1 gal = 4 qt |
Measures of Length
| Metric System | US Customary System | Conversions |
| Millimeter (mm) | Inch (in) | 1 in = 25.4 mm = 2.54 cm |
| Centimeter (cm) | Foot (ft) | 1 ft = 12 in = 30.48 cm |
| Meter (m) | Yard (yd) | 1 yd = 3 ft = .9144 m |
| Kilometer (km) | Mile (mi) | 1 mile = 5280 ft = 1760 yd = 1.6 km |
finger-like projections that line the small intestine
study of the relationships among genes, diet, and health outcomes
Identification of genetic markers that modify an individual's need for or use of various nutrients.
characteristic that increases the risk of developing a disease
"A healthy outside starts from the inside."
-Robert Urich (1946-2002), American actor
Human bodies change significantly over time, and food is the fuel for those changes. People of all ages need the same basic nutrients—amino acids, carbohydrates, fatty acids, vitamins and minerals, water—to sustain life and health. However, the amounts of nutrients needed differ. Throughout the human life cycle, the body constantly changes and goes through different periods known as stages. In this chapter we will discuss the major changes that occur during each stage, focusing on the roles nutrition plays. The major stages of the human life cycle are defined as follows:
- Pregnancy. The development of a zygote into an embryo and then into a fetus in preparation for childbirth.
- Infancy. The earliest part of childhood. It is the period from birth through age 1.
- Toddler years. Occur during ages 2 and 3 and are the end of early childhood.
- Childhood. Takes place from ages 4 to 8.
- Puberty. The period from ages 9 to 13, which is the beginning of adolescence.
- Older adolescence. The stage that takes place between ages 14 and 18.
- Adulthood. The period from adolescence to the end of life. Begins at age 19.
- Middle age. The period of adulthood that stretches from age 31 to 50.
- Senior years, or old age. Extends from age 51 until the end of life.
Learning Objectives
- Summarize prenatal nutritional requirements and dietary recommendations.
- Discuss the most important nutritional concerns during pregnancy.
- Discuss the benefits and barriers related to breastfeeding.
- Examine feeding problems that parents and caregivers may face with their infants.
- Explore the introduction of solid foods into a toddler’s diet.
- Discuss the most important nutrition-related concerns during childhood.
- Discuss the most important nutrition-related concerns during adolescence.
- Explain how nutritional and lifestyle choices can affect current and future health.
- Discuss the most important nutrition-related concerns during middle and old age.
18.1 Pregnancy
Conception to the Early Days of Pregnancy
Women who are trying to conceive should make proper dietary choices and practice healthy habits to ensure the delivery of a healthy baby. Fathers-to-be should also consider their lifestyles. For both men and women, a sedentary lifestyle, excess body weight, and a diet low in fresh fruits and vegetables may affect fertility. Men who consume too much alcohol, use certain drugs, and/or smoke cigarettes/use tobacco may also damage the quantity and quality of their sperm.1 For both men and women, adopting healthy habits also boosts general well-being and makes it possible to meet the demands of parenting.
Pregnancy is measured from the first day of a woman’s last menstrual period until childbirth, and typically lasts about 40 weeks. Humans like to think of pregnancy in terms of equal time, so we divide pregnancy into three approximately equal sections or trimesters. The first trimester is the first 13 weeks of pregnancy, the second is weeks 14 through 27, and pregnancy ends with the third trimester, weeks 28 through birth.
However, trimesters do not reflect the actual stages of development through the pregnancy. The first trimester encompasses several stages of development. At conception, a sperm cell fertilizes an egg cell, creating a zygote. This first stage of pregnancy accounts for the first 2 weeks. The zygote rapidly divides into multiple cells to become an embryo and implants itself in the uterine wall. Major changes begin to occur in these earliest days after conception, often weeks before a woman even knows that she is pregnant. The embryonic stage lasts from week 3 through week 10. During this time there are critical periods of development where the infrastructure for organ systems such as the nervous system, heart, limbs, ears, eyes, teeth, palate, and external genitalia is laid down. During these periods the developing embryo is very sensitive to damage caused by inadequate nutrition, medications, alcohol, or exposure to other harmful substances. Adequate nutrition supports cell division, tissue differentiation, and organ development, especially during these critical times. As each week passes, new milestones are reached. The end of the embryonic stage marks the start of the fetal stage which is week 11 through birth. During this stage the organ systems grow to maturity, and weight of the fetus increases from about 1 oz to about 7.5 lb. At the 20-week mark, physicians typically perform an ultrasound to acquire information about the fetus and check for abnormalities. By this time, it is possible to know the sex of the baby.
Good nutrition is vital for any pregnancy and not only helps an expectant mother remain healthy, but also impacts the development of the fetus and ensures that the baby thrives in infancy and beyond. During pregnancy, a woman’s needs increase for certain nutrients more than for others. If these nutritional needs are not met, infants could suffer from low birth weight (a birth weight less than 5.5 lb, or 2,500 grams), among other developmental problems. Therefore, it is crucial to make careful dietary choices.
Weight Gain during Pregnancy
During pregnancy, a mother’s body changes in many ways. One of the most notable and significant changes is weight gain. If a pregnant woman does not gain enough weight, her unborn baby will be at risk. Infant birth weight is one of the best indicators of a baby’s future health. Poor weight gain by the mother, especially in the third trimester, could result not only in low birth weight, but also in infant intellectual disabilities or mortality. Therefore, it is vital for a pregnant woman to maintain a healthy weight, and her weight prior to pregnancy also has a major effect. Pregnant women at a healthy weight pre-pregnancy should gain between 25-35 lb in total through the entire pregnancy. The precise amount that a mother should gain usually depends on her beginning body mass index (BMI).
Table 18.1.1 Recommended Weight Gain During Pregnancy
| Pre-Pregnancy BMI | Weight Category | Recommended Weight Gain |
| < 18.5 | Underweight | 28-40 lb |
| 18.5-24.9 | Healthy | 25-35 lb |
| 25.0-29.9 | Overweight | 15-25 lb |
| > 30.0 | Obese (all classes) | 11-20 lb |
Starting weight below or above the healthy range can lead to different complications. Pregnant women with a pre-pregnancy BMI below 20 kg/m2 are at a higher risk of a preterm delivery and an underweight infant. Pregnant women with a pre-pregnancy BMI above 30 kg/m2 have an increased risk of the need for a cesarean section during delivery. Therefore, it is optimal to have a BMI in the normal range prior to pregnancy.
Generally, women gain 2 to 5 lb in the first trimester. After that, it is recommended to gain no more than one lb per week until birth. Some of the new weight is due to the growth of the fetus, while some is due to changes in the mother’s body that support the pregnancy. Weight gain often breaks down in the following manner: 6 to 8 lb of fetus, 1 to 2 lb for the placenta (which supplies nutrients to the fetus and removes waste products), 2 to 3 lb for the amniotic sac (which contains fluids that surround and cushion the fetus), 1 to 2 lb in the breasts, 1 to 2 lb in the uterus, 3 to 4 lb of maternal blood, 3 to 4 lb maternal fluids, and 8 to 10 lb of extra maternal fat stores that will be needed for breastfeeding and delivery for a total of 25-35 lb. Women who are pregnant with more than one fetus are advised to gain even more weight to ensure the health of their unborn babies.
Weight Loss after Pregnancy
During labor, new mothers lose some of their gained weight (usually 9-13 lb) with the delivery of their child (weight of the baby, the placenta, and the amniotic fluid). In the following weeks, they continue to shed weight as they lose accumulated fluids and their blood volume returns to normal. Some studies have found that exclusive breastfeeding helps a new mother lose some of the extra weight when compared to non-exclusive breastfeeding.2
New mothers who gain the recommended amount of weight and participate in regular physical activity during their pregnancies have an easier time shedding weight post-pregnancy. However, women who gain more weight than needed for a pregnancy typically retain that excess weight as body fat. If that weight gain increases a new mother’s BMI by a unit or more, that could lead to complications such as hypertension or gestational diabetes in future pregnancies and later in life.
Nutritional Requirements
As a mother’s body changes, so do her nutritional needs. Pregnant women must consume more kcal and nutrients in the second and third trimesters than other adult women. However, the average recommended daily caloric intake can vary depending on activity level and the mother’s normal weight. Regardless, pregnant women should choose a high quality, diverse diet, consume fresh foods, and nutrient-rich meals. It is also standard for pregnant women to take prenatal supplements to ensure adequate intake of necessary micronutrients.
Energy and Macronutrients
During the first trimester, a pregnant woman has the same energy requirements as normal and should consume the same number of kcal as usual. However, as the pregnancy progresses, a woman must increase her caloric intake. A pregnant woman should consume an additional 340 kcal per day during the second trimester, and an additional 450 kcal per day during the third trimester.3 This is partly due to an increase in metabolism which rises during pregnancy. A woman can easily meet these increased needs by consuming more nutrient dense foods.
The recommended dietary allowance, or RDA, of carbohydrates during pregnancy is about 175 to 265 g per day to fuel fetal brain development. The best food sources for pregnant women include whole grain breads and cereals, brown rice, whole vegetables, legumes, and fruits. These and other unrefined carbohydrates provide nutrients, phytochemicals, antioxidants, and the extra 3 mg/day of fiber that is recommended during pregnancy. These foods also help to build the placenta and supply energy for the growth of the unborn baby.
During pregnancy, extra protein is needed for the synthesis of new maternal and fetal tissues. Protein builds muscle and other tissues, enzymes, antibodies, and hormones in both the mother and the unborn baby. Additional protein also supports increased blood volume and the production of amniotic fluid. Protein should be derived from healthy sources, such as lean red meat, poultry, legumes, nuts, seeds, eggs, and fish. Low-fat milk and other dairy products also provide protein, along with calcium and other micronutrients. To calculate protein needs during pregnancy, use pre-pregnancy weight in kg body weight times the RDA for protein (0.8 g/kg/day), and add 25 g. For example, if your pre-pregnancy weight was 150 lb:
- Convert 150 lb to kg by dividing by 2.2: 150 lb ÷ 2.2 lb/kg = 68 kg
- Multiply 68 kg by RDA: 68 kg x 0.8 g/kg/day = 54.5 g protein
- Add 25 g during second and third trimester: 54.5 g + 25 g = ~80 g protein
There are no specific recommendations for fats in pregnancy, apart from following normal dietary guidelines. However it is recommended to increase the amount of essential fatty acids (omega-3 and omega-6) because they are incorporated into the placenta and fetal tissues. Fats should make up 25-35% of daily kcal and should come from healthy sources, such as avocados, nuts and nut butters, and olives and olive oils. It is not recommended for pregnant women to be on a very low-fat diet, since it would be hard to meet the needs of essential fatty acids and fat soluble vitamins. Fatty acids are important during pregnancy because they support the baby’s brain and eye development.
Fluids
Fluid intake must also be monitored. According to the National Academy of Medicine (NAM), pregnant women should drink at least 2.3 liters (about 10 cups) of liquids per day to provide enough fluid for blood production.4 It is also important to drink additional liquids during physical activity or when it is hot and humid outside, to replace fluids lost via perspiration. The combination of a high fiber diet and lots of liquids also helps to eliminate waste.
Vitamins and Minerals
The daily requirements for women change with the onset of a pregnancy. Taking a daily prenatal supplement or multivitamin helps to meet many nutritional needs. However, most of these requirements should be fulfilled with a healthy diet. The following table compares the non-pregnant levels of required vitamins and minerals to the levels needed during pregnancy. For pregnant women, the RDA of nearly all vitamins and minerals increases.
Table 18.1.2 Recommended Micronutrient Intakes during Pregnancy
| Nutrient | Non-Pregnant Women | Pregnant Women |
| Vitamin A (mcg) | 700.0 | 770.0 |
| Thiamin (mg) | 1.1 | 1.4 |
| Riboflavin (mg) | 1.1 | 1.4 |
| Niacin (mg) | 14.0 | 18.0 |
| Vitamin B6 (mg) | 1.3 | 1.9 |
| Folate (mcg) | 400.0 | 600.0 |
| Vitamin B12 (mcg) | 2.4 | 2.6 |
| Vitamin C (mg) | 75.0 | 85.0 |
| Vitamin D (mcg) | 15.0 | 15.0 |
| Vitamin E (mg) | 15.0 | 15.0 |
| Calcium (mg) | 1000.0 | 1000.0 |
| Iron (mg) | 18.0 | 27.0 |
| Magnesium (mg) | 310.0 (19-30 yr) | 350.0 (19-30 yr) |
| 320.0 (31-50 yr) | 360.0 (31-50 yr) | |
| Phosphorus (mg) | 700.0 | 700.0 |
| Zinc (mg) | 8.0 | 11.0 |
The micronutrients involved with building the skeleton—vitamin D and calcium—are crucial during pregnancy to support fetal bone development. Although the recommended levels are the same as those for non-pregnant women, many women do not typically consume adequate amounts and should make an extra effort to meet those needs.
There is an increased need for all B vitamins during pregnancy. Adequate vitamin B6 supports the metabolism of amino acids, while more vitamin B12 is needed for the synthesis of red blood cells and DNA. Additional zinc is crucial for cell development and protein synthesis. The need for vitamin A also increases, and extra iron intake is important because of the increase in blood supply during pregnancy and to support the fetus and placenta. Iron needs increase by 1/3, and this increase is almost impossible to obtain in adequate amounts from food sources during pregnancy. Therefore, even if a pregnant woman consumes a healthy diet, there may still be a need to take an iron supplement, in the form of ferrous salts. Also remember that folate needs increase during pregnancy to 600 mcg per day to prevent neural tube defects (during the first 8 weeks of pregnancy). This micronutrient is also crucial because it helps produce the extra blood a woman’s body requires during pregnancy.
For other micronutrients, recommended intakes are the same as those for non-pregnant women, although it is crucial for pregnant women to make sure to meet the RDAs to reduce the risk of birth defects. In addition, pregnant mothers should avoid exceeding any recommendations. Taking megadose supplements can lead to excessive amounts of certain micronutrients, such as vitamin A and zinc, which may produce toxic effects that can also result in birth defects.
Guide to Eating during Pregnancy
Almost all of the modified energy and nutrient needs required during pregnancy can be met by consuming nutrient dense foods, which are essential to a healthy diet. Examples of nutrient dense foods include fruits, vegetables, whole grains, peas, beans, reduced-fat dairy, and lean meats. Pregnant women should be able to meet almost all of their increased needs via a healthy diet. However, as discussed previously, expectant mothers should take a prenatal supplement to ensure an adequate intake of iron and folate. Here are some additional dietary guidelines for pregnant women4:
- Eat iron-rich or iron-fortified foods, including meat or meat alternatives, breads, and cereals, to help satisfy increased need for iron and prevent anemia. Include vitamin C-rich foods, such as orange juice, broccoli, or strawberries, or peppers to enhance iron absorption.
- Eat a well-balanced diet including fruits, vegetables, whole grains, calcium-rich foods, lean meats, and a variety of cooked seafood (excluding fish that are high in mercury, such as swordfish and shark).
- Drink additional fluids, especially water.
Foods to Avoid
A number of substances can harm a growing fetus. Therefore, it is vital for women to avoid them throughout a pregnancy. Some are so detrimental that a woman should avoid them even if she suspects that she might be pregnant. For example, consumption of alcoholic beverages results in a range of abnormalities that fall under the umbrella of Fetal Alcohol Spectrum Disorders. They include learning and attention deficits, heart defects, and abnormal facial features. Alcohol enters the unborn baby via the umbilical cord and can slow fetal growth, damage the brain, or even result in miscarriage. The effects of alcohol are most severe in the first trimester, when the organs are developing. As a result, there is no safe amount of alcohol that a pregnant woman should consume.
Pregnant women should also limit caffeine intake, which is found not only in coffee, but also tea, colas, cocoa, chocolate, and some over-the-counter painkillers. Some studies suggest that very high amounts of caffeine have been linked to babies born with low birth weights. Most experts agree that small amounts of caffeine each day are safe for most pregnant women (approximately 200 mg/day or less)5 but check with your doctor.
For both mother and child, foodborne illness can cause major health problems. For example, the foodborne illness caused by the bacteria Listeria monocytogenes can cause spontaneous abortion and fetal or newborn meningitis. According to the Centers for Disease Control and Prevention (CDC), pregnant women are 10 times more likely to become infected with this disease than non-pregnant, healthy adults.6 Foods more likely to contain the bacteria and that should be avoided include unpasteurized dairy products, especially soft cheeses, smoked seafood, hot dogs, paté, cold cuts, and uncooked meats.
Pregnant women can eat fish, ideally 8 to 12 oz of different types each week. Expectant mothers are able to eat cooked shellfish such as shrimp, farm-raised fish such as salmon, and a maximum of 6 oz of albacore or white, tuna per week. However, they should avoid fish with high methylmercury levels, such as shark, swordfish, and king mackerel. (Please refer to Table 3.3.2 Mercury Levels in Fish in Chapter 3). Pregnant women should also avoid consuming raw fish to avoid foodborne illness.
Food Cravings and Aversions
Food aversions and cravings can occur during pregnancy and often get a lot of attention. Fortunately most do not have a major impact unless food choices are extremely limited. For most women, it is not harmful to indulge in the occasional craving, such as a desire for pickles and ice cream. However, a medical disorder known as pica, the craving and willing consumption of substances with little or no nutritive value, such as dirt, clay, or laundry starch, can be harmful. Pica is most prevalent among pregnant women and young children. Although the etiology (or cause) of pica is not completely understood, several studies have linked pica, particularly during pregnancy, to iron deficiency anemia.7
Physical Activity during Pregnancy
For most pregnant women, physical activity is a must and is recommended in the 2020 Dietary Guidelines for Americans. Regular exercise of moderate intensity, about 30 minutes per day most days of the week, keeps the heart and lungs healthy. It also helps to improve sleep and boosts mood and energy levels. In addition, women who exercise during pregnancy report fewer discomforts and may have an easier time losing excess weight after childbirth. Brisk walking, swimming, or an aerobics class geared toward expectant mothers are all great ways to get exercise during a pregnancy. Healthy women who already participate in vigorous activities, such as running, can continue doing so during pregnancy provided they discuss their exercise plan with their physicians.
However, pregnant women should avoid activities that could cause injury, such as soccer, football, and other contact sports, or activities that could lead to falls, such as horseback riding and downhill skiing. It may be best for pregnant women not to participate in certain sports, such as tennis, that require you to jump or change direction quickly. Scuba diving should also be avoided because it might result in the fetus developing decompression sickness.
Complications during Pregnancy
Expectant mothers may face different complications during the course of their pregnancy. They include certain medical conditions that could greatly impact a pregnancy if left untreated, such as gestational hypertension and gestational diabetes, which have diet and nutrition implications.
Gestational Hypertension
Gestational hypertension is a condition of high blood pressure during the second half of pregnancy. First time mothers are at a greater risk, along with women who have mothers or sisters who had gestational hypertension, women carrying multiple fetuses, women with a prior history of high blood pressure or kidney disease, and women who are overweight or obese when they become pregnant. Hypertension can prevent the placenta from getting enough blood, which would result in the baby getting less oxygen and nutrients. This can result in low birth weight, although most women with gestational hypertension can still deliver a healthy baby if the condition is detected and treated early.
Some risk factors for gestational hypertension can be controlled such as diet, while others cannot, such as family history. If left untreated, gestational hypertension can lead to a serious complication called preeclampsia, which is sometimes referred to as toxemia. This disorder is marked by elevated blood pressure, protein in the urine, and is associated with fluid retention and swelling. If preeclampsia worsens, a life-threatening condition for both the mother and the baby called eclampsia can occur.
Gestational Diabetes
About 8% of pregnant women suffer from a condition known as gestational diabetes, or abnormal glucose tolerance during pregnancy.8 As discussed in Chapter 5, gestational diabetes is similar to type 2 diabetes. The mother's body becomes resistant to the hormone insulin, which enables cells to transport glucose from the blood and into cells. Gestational diabetes is typically diagnosed between 24-28 weeks using a glucose tolerance test, although it is possible for the condition to develop later into a pregnancy. Signs and symptoms include extreme hunger, thirst, or fatigue. The excess glucose in the mother's blood is transported to the placenta, and the fetus will take up this excess glucose from the mother. If blood glucose levels are not properly monitored and treated, the baby might gain too much weight, possibly causing a premature birth and/or a difficult delivery. Diet and regular physical activity can help to manage this condition. Some patients with gestational diabetes may require daily insulin injections to boost the absorption of glucose from the bloodstream and promote the storage of glucose in the form of glycogen in liver and muscle cells. Gestational diabetes usually resolves quickly after childbirth, however women who suffer from this condition have a 50% chance of eventually developing type 2 diabetes later in life, particularly if they are overweight.
18.2 Breastfeeding
After the birth of the baby, nutritional needs must be met to ensure that an infant not only survives, but thrives from infancy into childhood. Exclusive breastfeeding is one of the best ways a mother can support the growth and protect the health of her infant child.
Breast milk contains all of the nutrients that a newborn requires for rapid growth and development and gives a child the best start to a healthy life. New mothers must consider their own nutritional requirements to help their bodies recover in the wake of the pregnancy and delivery. This is particularly true for women who breastfeed their babies, which calls for an increased intake of certain nutrients.
Benefits of Breastfeeding
Breastfeeding has a number of benefits, both for the mother and for the child. Breast milk contains immunoglobulins, enzymes, immune factors, and white blood cells. As a result, breastfeeding boosts the baby’s immune system and lowers the incidence of diarrhea, along with respiratory diseases, gastrointestinal problems, and ear infections. Breastfed babies also are less likely to develop asthma and allergies, and breastfeeding lowers the risk of sudden infant death syndrome (SIDS). In addition, human milk encourages the growth of healthy bacteria in an infant’s intestinal tract. All of these benefits remain in place long after an infant has been weaned from breast milk. Some studies suggest other possible long-term effects. For example, breast milk may protect against type 1 diabetes and obesity, although research is ongoing in these areas.9
Breastfeeding has a number of other important benefits. It is easier for babies to digest breast milk than bottle formula, which often contains proteins made from cow’s milk that require an adjustment period for infant digestive systems. Breastfed infants are sick less often than formula-fed infants. Breastfeeding is more sustainable and results in less plastic waste and other trash. Breastfeeding can also save families money because it does not incur the same cost as purchasing formula. Breast milk is always ready. It does not have to be mixed, heated, or prepared. Also, breast milk is sterile and always at the right temperature. In addition, the skin-to-skin contact of breastfeeding promotes a close bond between mother and baby, which provides important emotional and psychological benefits. The practice also provides health benefits for the mother. Studies have shown that breastfeeding reduces the risk of type 2 diabetes, and breast and ovarian cancers for the mother.9
The choice to breastfeed is one that all new mothers face. Although breast milk is ideal for almost all infants, there are some challenges that nursing mothers may face when starting and continuing to breastfeed their infants. These obstacles include painful engorgement or fullness in the breasts, sore and tender nipples, lack of comfort or confidence in public, and lack of accommodation to breastfeed or express milk in the workplace. Support from family members, friends, employers, and others can greatly help with both the decision making process during pregnancy and the practice of breastfeeding after the baby’s birth. In the US in 2015, about 83% of babies started out being breastfed. Yet by the age of six months, when solid foods should begin to be introduced, only 24% of infants were still breastfed exclusively. Employed mothers have been less likely to initiate breastfeeding and tend to breastfeed for a shorter period of time than new mothers who are not employed outside the home or who have lengthy maternity leaves.10 Around the world, less than 40% of infants under the age of six months are breastfed exclusively.11
International Board Certified Lactation Consultants are healthcare professionals (often a registered nurse or registered dietitian) certified in breastfeeding management that work with new mothers to solve problems and educate families about the benefits of this practice. Women who give birth in hospitals with lactation consultants are more likely to breastfeed. Once a new mother has left the hospital for home, she also needs access to a trained individual who can provide consistent information.12 Lactation consultants can help new mothers learn proper technique, and help troubleshoot breastfeeding problems when they occur.
Affordable Care Act and Breastfeeding
In 2010 in the US, the passage of the Affordable Care Act (ACA) called for employers to provide accommodations within the workplace for new mothers to pump breast milk. This law requires a private and clean space within the workplace, other than a restroom, along with adequate break time for a woman to express milk. Yet as of 2018 only 49% of employers provided worksite lactation support programs.10
Contraindications to Breastfeeding
Although there are numerous benefits to breastfeeding, in some cases there are also risks that must be considered. A new mother with HIV should not breastfeed as the infection can be transmitted through breast milk. Breastfeeding is also not recommended for women undergoing radiation or chemotherapy treatment for cancer. Women actively using alcohol excessively and/or illicit drugs should also avoid breastfeeding.
Lactation
Lactation (or lactogenesis) is the synthesis and secretion of breast milk. An infant suckling at the breast stimulates nerve endings which signal the pituitary gland to release two hormones, prolactin and oxytocin. Prolactin signals the growth of the milk duct system and initiates and maintains milk production in the alveoli of the breast.
Oxytocin is involved in milk ejection, also called milk letdown. It signals contraction of the alveoli cells, forcing milk into the ducts and out through the nipple. The nipple tissue becomes firmer with stimulation, which makes it more flexible and easier for the baby to grasp in the mouth. The release of oxytocin also has psychological benefits by inducing calm and enhancing feelings of affection or bonding between mother and baby.13
New mothers need to adjust their caloric and fluid intake to make breastfeeding possible. The RDA is 330 additional kcal per day during the first six months of lactation and 400 additional kcal during the second six months of lactation. The energy needed to support breastfeeding comes from both increased intake and from stored fat. For example, during the first six months after her baby is born, the daily caloric cost for a lactating mother is 500 kcal, with 330 kcal derived from increased intake and 170 kcal derived from maternal fat stores. This helps explain why breastfeeding may promote weight loss in new mothers. Lactating women should also drink approximately 13 cups of liquids per day to maintain milk production, according to the NAM. As is the case during pregnancy, the RDA of several vitamins and minerals increases for women who are breastfeeding their babies. The following table compares the recommended vitamins and minerals for lactating women to the levels for non-pregnant and pregnant women.
Table 18.2.1 Recommended Micronutrient Intakes during Pregnancy
| Nutrient | Non-Pregnant Women | Pregnant Women | Lactating Women |
| Vitamin A (mcg) | 700.0 | 770.0 | 1300.0 |
| Thiamin (mg) | 1.1 | 1.4 | 1.4 |
| Riboflavin (mg) | 1.1 | 1.4 | 1.6 |
| Niacin (mg) | 14.0 | 18.0 | 17.0 |
| Vitamin B6 (mg) | 1.3 | 1.9 | 2.0 |
| Folate (mcg) | 400.0 | 600.0 | 500.0 |
| Vitamin B12 (mcg) | 2.4 | 2.6 | 2.8 |
| Vitamin C (mg) | 75.0 | 85.0 | 120.0 |
| Vitamin D (mcg) | 15.0 | 15.0 | 15.0 |
| Vitamin E (mg) | 15.0 | 15.0 | 19.0 |
| Calcium (mg) | 1000.0 | 1000.0 | 1000.0 |
| Iron (mg) | 18.0 | 27.0 | 9.0 |
| Magnesium (mg) | 310.0 (19-30 yr) | 350.0 (19-30 yr) | 310.0 (19-30 yr) |
| 320.0 (31-50 yr) | 360.0 (31-50 yr) | 320.0 (31-50 yr) | |
| Phosphorus (mg) | 700.0 | 700.0 | 700.0 |
| Zinc (mg) | 8.0 | 11.0 | 12.0 |
Calcium requirements do not change during breastfeeding because of more efficient absorption, which is the case during pregnancy, as well. However, the reasons for this differ. During pregnancy, there is enhanced absorption of calcium within the gastrointestinal tract. During lactation, there is enhanced retention by the kidneys. The RDA for phosphorus, vitamin D, and fluoride also remain the same. The RDA for iron is reduced significantly during lactation to half of the requirement for non-pregnant women. This is because, for most women, lactation significantly reduces or eliminates menstruation.
Components of Breast Milk
Human breast milk not only provides adequate and highly bioavailable nutrition for infants, it also helps to protect newborns from disease. Breast milk is rich in cholesterol, which is needed for brain development. Colostrum is produced immediately after birth, prior to the start of milk production, and lasts for several days after the arrival of the baby. Colostrum is thicker than breast milk, and is often yellowish in color. This protein-rich liquid fulfills an infant’s nutrient needs during those early days. Although low in volume, colostrum is packed with concentrated nutrition for newborns. This special "milk" is high in fat-soluble vitamins, minerals, and immunoglobulins (antibodies) that pass from the mother to the baby. Immunoglobulins provide passive immunity for the newborn and protect the baby from bacterial and viral diseases.14
Two to four days after birth, colostrum is replaced by transitional milk. Transitional milk is a creamy liquid that lasts for approximately two weeks and includes high levels of fat, lactose, and water soluble vitamins. It also contains more kcal than colostrum.
Mature milk is the final fluid that a new mother produces. In most women, this begins by the end of the second week postpartum. There are two types of mature milk that appear during a feeding. Foremilk occurs at the beginning and includes more water, vitamins, and protein. Hindmilk occurs after the initial release of milk and contains higher levels of fat, which is necessary for weight gain. Combined, these two types of milk ensure that a baby receives adequate nutrients to grow and develop properly.15
About 90% of mature milk is water, which helps an infant remain hydrated. The remaining 10% contains carbohydrates, proteins, and fats, which support energy and growth. Similar to cow’s milk, the main carbohydrate of mature breast milk is lactose. Breast milk contains vital essential fatty acids, such as docosahexaenoic acid (DHA) and arachidonic acid (ARA). In terms of protein, breast milk contains more whey than casein (which is the reverse of cow’s milk). Whey is much easier for infants to digest than casein. Complete protein, which means all of the essential amino acids, is also present in breast milk, as well as lactoferrin, an iron-gathering compound that helps to absorb iron into an infant’s bloodstream.
In addition, breast milk provides adequate vitamins and minerals. Although absolute amounts of some micronutrients are low, they are more efficiently absorbed by infants. Other essential components include digestive enzymes that help a baby digest the breast milk. Human milk also provides the hormones and growth factors that help a newborn to develop.
Diet and Milk Quality
A mother’s diet can have a major impact on milk production and quality. As during pregnancy, lactating mothers should avoid harmful substances such as tobacco. Some legal drugs and herbal products can be harmful as well, so it is important to discuss them with a healthcare provider. Some mothers may need to avoid certain things, such as spicy foods, that can produce gas in sensitive infants. Avoiding alcohol completely is the safest option for a breastfeeding mother. However, consumption of up to one alcoholic drink a day (12 oz of beer, 5 oz of wine, or 1.5 oz of liquor) is not known to be harmful to the infant, particularly if the mother waits 2-3 hours after consumption to breastfeed.16
In terms of the mother’s nutrient intake, there is limited research regarding the extent of its role on breast milk composition. A systematic review of 36 journal publications found that the concentration of fatty acids and vitamins A, C, B6, and B12 are reported to be most influenced by maternal diet, while mineral content is much less affected.17 However, more research on this topic is needed.
Bottle Formula Feeding
Most women can and should breastfeed when given sufficient education and support. However, as discussed, a small percentage of women are unable to breastfeed their infants, while others choose not to. While infant formula provides a balance of nutrients, not all formulas are the same and there are important considerations that parents and caregivers must weigh. Standard formulas use cow’s milk as a base. They have 20 kcal per fl oz, similar to breast milk, with vitamins and minerals added. Cow’s milk alone should never be given to babies under the age of one as young infants cannot fully digest it and it does not meet their nutrient needs. Soy-based formulas are usually given to infants who develop diarrhea, constipation, vomiting, colic, or abdominal pain, or to infants with a cow’s milk protein allergy.
Hypoallergenic protein hydrolysate formulas are usually given to infants who are allergic to cow’s milk and soy protein. This type of formula uses hydrolyzed protein, meaning that the protein is already broken down into amino acids and small peptides, which makes it easier to digest. Preterm infant formulas are given to low birth weight infants, if breast milk is unavailable. Preterm infant formulas have 24 kcal per fl oz and are given until the infant reaches a desired weight.
Infant formula comes in three basic types:
- Powder that requires mixing with water. This is the least expensive type of formula.
- Concentrates, which are liquids that must be diluted with water. This type is slightly more expensive.
- Ready-to-use liquids that can be poured directly into bottles. This is the most expensive type of formula. However, it requires the least amount of preparation. Ready-to-use formulas are also convenient for traveling.
Most babies need about 2.5 oz of formula per lb of body weight each day. Therefore, the average infant should consume about 24 fl oz of breast milk or formula per day. When preparing formula, parents and caregivers should carefully follow the safety guidelines, since an infant has an immature immune system. All equipment used in formula preparation should be sterilized. Prepared, unused formula should be refrigerated to prevent bacterial growth. Parents should make sure not to use contaminated water to mix formula in order to prevent foodborne illnesses. Follow the instructions for powdered and concentrated formula carefully. Formula that is overly diluted would not provide adequate kcal and protein, while overly concentrated formula provides too much protein and too little water which can impair kidney function.
It is important to note again that both the American Academy of Pediatrics and the World Health Organization (WHO) state that breast milk is far superior to infant formula. This table compares some of the advantages of giving a child breast milk to the disadvantages of using bottle formula.
Table 18.2.2 Breast Milk vs. Bottle Formula
| Breast Milk | Bottle Formula |
| Antibodies and lactoferrin in breast milk protect infants. | Formula does not contain immunoprotective factors. |
| The iron in breast milk is absorbed more easily. | Formula contains more iron than breast milk but it is less easily absorbed. |
| The feces that breastfed babies produce lacks smell due to different bacteria in the gut. | The feces that formula fed infants produce tends to have more of a foul odor. |
| Breast milk is always available and is always at the correct temperature. | Formula must be prepared, refrigerated for storage and warmed before given to an infant. |
| Breastfed babies are less likely to have constipation. | Formula fed babies tend to have more constipation. |
| Breastfeeding ostensibly is free, though purchasing a pump and bottles to express milk does require some expense. | Formula must be purchased and is expensive. |
| Breast milk contains the essential fatty acids, DHA and ARA, which are critical for brain and vision development. | Some formulas contain DHA and ARA. |
18.3 Infancy
Diet and nutrition have a major impact on a child’s development from infancy into the adolescent years. A healthy diet not only affects growth, but also immunity, intellectual capabilities, and emotional well-being. One of the most important jobs of parenting is making sure that children receive an adequate amount of needed nutrients to provide a strong foundation for the rest of their lives.
Infant Growth and Development
A number of major physiological changes occur during infancy. The trunk of the body grows faster than the arms and legs, while the head becomes less prominent in comparison to the limbs. Organs and organ systems grow at a rapid rate. Also during this period, countless new synapses form to link brain neurons. Two soft spots on the baby’s skull, known as fontanels, allow the skull to accommodate rapid brain growth. The posterior fontanel closes first, by eight weeks of age. The anterior fontanel closes about a year later, at 18 months on average. Developmental milestones include sitting up without support, learning to walk, teething, and vocalizing among many, many others. All of these changes require adequate nutrition to ensure development at the appropriate rate.18
Healthy infants grow steadily, but not always at an even pace. For example, during the first year of life, height increases by 50%, while weight triples. Physicians and other health professionals use growth charts to track a baby’s development process. Because infants cannot stand, length is used instead of height to determine the rate of a child’s growth. Other important developmental measurements include head circumference and weight. All of these must be tracked and compared against standard measurements for an infant’s age.
For infants and toddlers, the WHO growth charts are used to monitor growth. These standards represent optimal growth for children at this age and allow for tracking growth trends over time through percentile rankings. Growth charts may provide warnings that a child has a medical problem or is malnourished. Insufficient weight or height gain during infancy may indicate a condition known as failure-to-thrive, which is characterized by poor growth.
Nutritional Requirements
Requirements for macronutrients and micronutrients on a per kg basis are higher during infancy than at any other stage in the human life cycle. These needs are affected by the rapid cell division that occurs during growth, which requires energy and protein, along with the nutrients that are involved in DNA synthesis. During this period, children are entirely dependent on their parents or other caregivers to meet these needs. For almost all infants, six months or younger, breast milk is the best source to fulfill nutritional requirements. An infant may require feedings 8-12 times a day or more in the beginning. After six months, infants can gradually begin to consume solid foods to help meet nutrient needs.
Energy and Macronutrients
Energy needs relative to size are much greater in an infant than an adult. A baby’s resting metabolic rate is two times that of an adult. The RDA to meet energy needs changes as an infant matures and puts on more weight. Just as we calculate energy needs in adults using various equations, there are also equations to calculate total energy expenditure and resulting energy needs for infants and children. For example, the equation for the first three months of life is: (89 x weight [kg] − 100) + 175 kcal. However, the amount and frequency an infant wants to eat will also change over time due to growth spurts, which typically occur at about two and six weeks of age, and again at about three months and six months of age.
The dietary recommendations for infants are based on the nutritional content of human breast milk. Carbohydrates make up about 45-65% of the caloric content in breast milk, which amounts to an RDA of about 130 g. Almost all of the carbohydrate in human milk is lactose, which infants digest and tolerate well. In fact, lactose intolerance is practically nonexistent in infants (not to be confused with an allergy to the protein in cow's milk). Protein makes up about 5-20% of the caloric content of breast milk, which amounts to about 13 g per day. Infants need protein to support growth and development, though excess protein (which is only a concern with formula feeding) can cause dehydration, diarrhea, fever, and acidosis in premature infants. About 30-40% of the caloric content in breast milk is made up of fat. A high fat diet is necessary to encourage the development of neural pathways in the brain and other parts of the body. However, saturated fats and trans fatty acids inhibit this growth. Infants who are over the age of six months, which means they are no longer exclusively breastfed, should not consume foods that are high in these types of fats.
Micronutrients
Almost all of the nutrients that infants require can be met if they consume an adequate amount of breast milk. There are a few exceptions, though. Human milk is low in vitamin D, which is needed for calcium absorption and building bone, among other things. Therefore, breastfed children often need to take a vitamin D supplement in the form of drops. Infants at the highest risk for vitamin D deficiency are those with darker skin and/or no exposure to sunlight. Breast milk is also low in vitamin K, which is required for blood clotting, and deficits could lead to bleeding or hemorrhagic disease. Babies are born with limited vitamin K. Since 1961, the American Academy of Pediatrics has recommended newborns be given a low dose vitamin K injection shortly after birth.19
Breast milk is not high in iron, but the iron in breast milk is well absorbed by infants. Babies are born with about a six month supply of stored iron. After six months, however, an infant needs an additional source of iron other than breast milk. This is typically the time solid foods begin to be introduced, particularly iron-enriched cereals.20
Fluids
Infants have a high need for fluids, 1.5 ml per kcal consumed compared to 1.0 ml per kcal consumed for adults. This is because children have larger body surface area per unit of body weight and a reduced capacity for perspiration. Therefore, they are at greater risk of dehydration. However, parents or other caregivers can meet an infant’s fluid needs with breast milk or formula. As solids are introduced, parents must make sure that young children continue to drink fluids throughout the day.
Introducing Solid Foods
The American Academy of Pediatrics and the WHO recommends exclusive breastfeeding for the first six months of life, followed by continued breastfeeding as complementary foods are introduced, with continuation of breastfeeding for one year or longer as mutually desired by mother and infant.14
Infants should not exclusively consume solid foods prior to six months as these do not contain the right nutrient mix that infants need. If parents try to feed an infant who is too young or is not ready, their tongue will push the food out, which is called an extrusion reflex. Further, research suggests that infants who are fed solid foods too soon are more susceptible to developing food allergies. A child may be ready to eat solids, once they can sit with little or no support, has good head control, and opens their mouth and leans toward food when it is offered.20
Solid baby foods can be bought commercially or prepared from regular food using a food processor, blender, food mill, or grinder at home. By nine months to a year, infants are able to chew soft foods and can eat solids that are well chopped or mashed. It is important to feed a young child only one new food at a time, to help identify allergic responses or food intolerances. An iron supplement or iron-fortified cereal is still recommended at this time.
18.4 Toddler Years
Major physiological changes continue into the toddler years. Unlike in infancy, the limbs grow much faster than the trunk, which gives the body a more proportionate appearance. By the end of the third year, a toddler is taller and more slender than an infant, with a more erect posture. As the child grows, bone density increases and bone tissue gradually replaces cartilage.
Developmental milestones include running, drawing, toilet training, and self-feeding. How a toddler acts, speaks, learns, and eats offers important clues about their development. By the age of two, children have advanced from infancy and are on their way to becoming school-aged children. Their physical growth and motor development slows compared to the progress they made as infants. However, toddlers experience enormous intellectual, emotional, and social changes. Of course, food and nutrition continue to play an important role in a child’s development. During this stage, the diet completely shifts from breastfeeding or formula feeding to solid foods along with other liquids. Parents of toddlers also need to be mindful of certain nutrition-related issues that may crop up during this stage of the human life cycle. For example, fluid requirements relative to body size are higher in toddlers than in adults because children are at greater risk of dehydration.
The toddler years pose interesting challenges for parents or other caregivers, as children learn how to eat on their own and begin to develop personal preferences.
Nutritional Requirements
A toddler’s serving sizes should be approximately one-quarter that of an adult serving size. One way to estimate serving sizes for young children is one tablespoon for each year of life. For example, a 2 year old child would be served 2 tbsp of fruits or vegetables at a meal, while a 4 year old would be given 4 tbsp, or one-quarter cup. Here is an example of a toddler-sized meal:
- 1 oz of meat or chicken, or 2 to 3 tbsp of beans
- 1/4 slice of whole-grain bread
- 1 to 2 tbsp of cooked vegetable
- 1 to 2 tbsp of fruit
Energy
The energy requirements for ages two to three are about 1,000-1,400 kcal a day. In general, a toddler needs to consume about 40 kcal for every inch of height. For example, a young child who measures 32 inches should take in an average of 1,300 kcal a day. However, the recommended caloric intake varies with each child’s level of activity. Toddlers require small, frequent, nutritious snacks and meals to satisfy energy requirements. The amount of food a toddler needs from each food group depends on daily kcal needs. See Table 18.4.1 for serving size guidelines.
Table 18.4.1 Serving Sizes for Toddlers21
| Food Group | 2 Year olds | 3 Year olds | What Counts as: |
| Fruit | 1 c | 1-1½ c | ½ cup of fruit?
|
| Vegetables | 1 c | 1-1½ c | ½ cup of veggies?
|
| Grains | 3 oz | 3-5 oz | 1 oz grain?
|
| Protein Foods | 2 oz | 2-4 oz | 1 oz protein food?
|
| Dairy | 2 c | 2-2½ c | ½ cup dairy?
|
Macronutrients
Toddlers’ needs increase to support their body and brain development. For toddlers, the AMDR for carbohydrate intake is 45-65% of daily kcal. For protein, it's 5-20% and for fat it's 30-40% of daily kcal. Essential fatty acids are vital for the development of the eyes, along with nerves and other types of tissue. However, toddlers should not consume foods with high amounts of trans fats and saturated fats. Instead, young children require the equivalent of three teaspoons of healthy oils, such as olive oil, each day.
Micronutrients
As a child grows bigger, the demands for micronutrients increase. These needs for vitamins and minerals can be met with a balanced diet, with a few exceptions. According to the American Academy of Pediatrics, toddlers and children of all ages need 15 mcg of vitamin D per day. Vitamin D-fortified milk and cereals can help to meet this need. However, toddlers who do not get enough of this micronutrient should receive a supplement. Pediatricians may also prescribe a fluoride supplement for toddlers who live in areas with fluoride-poor water.
Iron deficiency is also a major concern for children between the ages of two and three. Iron deficiency anemia (IDA) can cause a number of problems including weakness, pale skin, shortness of breath, fatigue, and irritability. It can also result in intellectual, behavioral, or motor problems. IDA can occur as young children are weaned from iron-rich foods, such as breast milk and iron-fortified formula. They begin to eat solid foods that may not provide enough of this nutrient. Therefore, it is important that parents and caregivers add more iron-rich foods to a child’s diet, including lean meats, fish, poultry, eggs, legumes, and iron-enriched whole-grain breads and cereals. Children may also be given a daily supplement, such as ferrous sulfate drops.
Food-Related Problems in the Toddler Years
During the toddler years, parents may face a number of problems related to food and nutrition. Possible obstacles include difficulty helping a young child overcome a fear of new foods, or fights over messy habits at the dinner table. Even in the face of problems and confrontations, parents and other caregivers must make sure their preschooler has nutritious choices at every meal. For example, even if a child stubbornly resists eating vegetables, parents should continue to provide them. Before long, the child may change their mind, and develop a taste for foods once abhorred. It is important to remember this is the time to establish or reinforce healthy habits.
Registered Dietitian Ellyn Satter states that feeding is a responsibility that is split between parent and child. According to Satter and her Division of Responsibility in Feeding, parents are responsible for what their infants eat, while infants are responsible for how much they eat. In the toddler years and beyond, parents are responsible for what children eat, when they eat, and where they eat, while children are responsible for how much food they eat and whether they eat. Satter states that the role of a parent or a caregiver in feeding includes the following22:
- selecting and preparing food
- providing regular meals and snacks
- making mealtimes pleasant
- showing children what they must learn about mealtime behavior
- being considerate of children's lack of food experiences without catering to likes and dislikes
Picky Eaters
Children at this stage are often picky about what they want to eat. They may turn their heads away after eating just a few bites. Or they may resist coming to the table at mealtimes. They also can be unpredictable about what they want to consume for specific meals or at particular times of the day. Although it may seem as if toddlers should increase their food intake to match their level of activity, there may be a good reason for picky eating. A child’s growth rate slows after infancy, and toddlers do not require as much food.
Some children may also go through a food jag, or period of time where they only want to eat the same few foods every day and for most, if not every, meal. While this can be a way for a child to begin to express some independence, which is a normal part of development, it can make for frustrating meal times. It's important not to force a child to eat foods they don't want as this can actually prolong the food jag. Instead, offer new foods or healthy foods that they like and allow them to eat the preferred food with remaining food on their plate. Remember to follow Ellyn Satter's Division of Responsibility in Feeding as stated above.
Choking
At this young age, children are still learning how to adequately chew and swallow, increasing the risk of choking. To minimize this risk, encourage children to sit when eating, chew thoroughly, play close attention to what they put in their mouths, and supervise older children who may give foods considered choking hazards to younger kids. Such foods include nuts, whole cherries or grapes, raw carrots or celery, hard candy, hot dogs, etc. Make sure to cut foods into smaller and/or mashed pieces.
Early Childhood Caries
Early childhood caries (dental issues such as cavities) remain a potential problem during the toddler years. The risk of early childhood caries increases with the consumption of foods with a higher sugar content. According to the National Health and Nutrition Examination Survey, children between ages of 2 and 5 consume slightly more than 200 kcal of added sugar per day or approximately 13% of their total kcal.26 This is much more than recommended. Therefore, parents with toddlers should avoid processed foods, such as snacks from vending machines, and sugary beverages, such as soda. Parents also need to instruct a child on brushing their teeth at this time to help a toddler develop healthy habits and avoid tooth decay.
Toddler Obesity
Another potential problem during the early childhood years is toddler obesity. According to the WHO, the number of overweight or obese infants and young children (five years and younger) has increased from 32 million globally in 1990 to 41 million in 2016.23 In the US, the proportion of obese two to five year-olds increased from 5% in the 1970s to 13.9% in 2015.24,25
Obesity during early childhood tends to linger as a child matures and can cause health problems later in life. Recall from Chapter 9 that children undergo both hyperplasia and hypertrophy of adipose tissue, and the additional adipose cells created during childhood remain in adulthood. There are a number of reasons for the increases in obesity rates in toddlers. One is a lack of time. Parents and other caregivers who are constantly on the go may find it difficult to fit home-cooked meals into a busy schedule and may turn to fast food and other conveniences that are quick and easy, but not nutritionally sound. Another contributing factor is a lack of access to fresh fruits and vegetables. This is a problem particularly in low-income neighborhoods where local stores and markets may not stock fresh produce or may have limited affordable options. Physical inactivity is also a factor, as toddlers who live a sedentary lifestyle are more likely to be overweight or obese. Another contributor is a lack of breastfeeding support. Children who were breastfed as infants show lower rates of obesity than children who were formula-fed.
To prevent or address toddler obesity parents and caregivers can do the following:
- Eat at the kitchen table instead of in front of a television to monitor what and how much a child eats.
- Offer a child healthy portions. The size of a toddler’s fist is an appropriate serving size.
- Toddlers should be physically active throughout the day, with no more than 60 minutes of sedentary activity, such as watching television, per day.
Food for Thought
What would you recommend to help families prevent obesity among their children? What tips would you provide? What lifestyle changes might help?
18.5 Childhood
Nutritional needs change as children leave the toddler years. From ages four to eight, school-aged children grow consistently, but at a slower rate than infants and toddlers. They also experience the loss of deciduous, or “baby” teeth, and the arrival of permanent "adult" teeth, which typically begins at age six or seven. As new teeth come in, many children have some malocclusion, or malposition, of their teeth, which may affect their ability to chew food. Other changes that affect nutrition include the influence of peers on dietary choices and the kinds of foods offered by schools and after-school programs, which can make up a sizable part of a child’s diet. Excessive weight gain early in life can lead to obesity into adolescence and adulthood.
At this life stage, a healthy diet facilitates physical and mental development and helps to maintain health and wellness. School-aged children experience steady, consistent growth, with an average growth rate of 2 to 3 inches in height and 4.5 to 6.5 lb in weight per year. In addition, the rate of growth for the extremities is faster than for the trunk, which results in more adult-like proportions.
Nutritional Requirements
Energy
Children’s energy needs vary depending on their growth and level of physical activity. Energy requirements may also vary according to biological sex. Girls ages 4 to 8 require 1,200-1,800 kcal a day, while boys need 1,200-2,000 kcal daily and, depending on their activity level, a child may require more. Also, recommended intakes of macronutrients and most micronutrients are higher relative to body size, compared with nutrient needs during adulthood.
Macronutrients
For carbohydrates, the AMDR remains 45-65% of daily kcal. Children also require 17-25 g of fiber per day. They have a high need for protein to support muscle growth and development, therefore the AMDR increases a bit to 10-30% of daily kcal. High levels of essential fatty acids are needed to support growth (although not as high as in infancy and toddler years). As a result, the AMDR for fat is 25-35% of daily kcal.
Micronutrients
Micronutrient needs should be met with foods first. Parents and caregivers should select a variety of foods from each food group to ensure that nutritional requirements are met. Because children grow rapidly, they require foods that are high in iron, such as lean meats, legumes, fish, poultry, and iron-enriched cereals. Adequate fluoride is crucial to support strong teeth. Two of the most important micronutrient requirements during childhood are adequate calcium and vitamin D intake. Both are needed to build dense bones and a strong skeleton. Children who do not consume adequate vitamin D should be given a supplement of 10 mcg per day. Table 18.5.1 shows the micronutrient recommendations for school-aged children. Note that the recommendations are the same for boys and girls. As we progress through the different stages of the human life cycle, there will be some differences between males and females regarding micronutrient needs.
Table 18.5.1 Recommended Micronutrient Intakes during Childhood
| Nutrient | 4-8 Years | 9-13 Years |
| Vitamin A (mcg) | 400.0 | 600.0 |
| Thiamin (mg) | 0.6 | 0.9 |
| Riboflavin (mg) | 0.6 | 0.9 |
| Niacin (mg) | 8.0 | 12.0 |
| Vitamin B6 (mg) | 0.6 | 1.0 |
| Folate (mcg) | 200.0 | 200.0 |
| Vitamin B12 (mcg) | 1.2 | 1.8 |
| Vitamin C (mg) | 25.0 | 45.0 |
| Vitamin D (mcg) | 15.0 | 15.0 |
| Vitamin E (mg) | 7.0 | 11.0 |
| Vitamin K (mcg) | 55.0 | 60.0 |
| Calcium (mg) | 1000.0 | 1300.0 |
| Iron (mg) | 10.0 | 8.0 |
| Magnesium (mg) | 130.0 | 240.0 |
| Phosphorus (mg) | 500.0 | 1250.0 |
| Selenium (mcg) | 30.0 | 40.0 |
| Zinc (mg) | 5.0 | 8.0 |
Factors Influencing Intake
A number of factors can influence children’s eating habits and attitudes toward food. Family environment, societal trends, taste preferences, and messages in the media all impact the emotions that children develop in relation to their diet. Television commercials can entice children to consume sugary products, fatty fast foods, excess kcal, refined ingredients, and sodium. Therefore, it is critical that parents and caregivers direct children toward healthy choices.
One way to encourage children to eat healthy foods is to make meals and snacks fun and interesting. Parents should include children in food planning and preparation, for example selecting items while grocery shopping or helping to prepare part of a meal, such as making a salad. At this time, parents can also educate children about kitchen safety. It might be helpful to cut sandwiches, meats, or pancakes into small or interesting shapes. In addition, parents should offer nutritious desserts, such as fresh fruits, instead of calorie-laden cookies, cakes, salty snacks, and ice cream. Additionally, research has found that regularly eating dinner as a family is associated with greater consumption of fruits, vegetables, and less saturated and trans fat.27
18.6 Adolescence
The onset of puberty is the beginning of adolescence and is the bridge between the childhood years and young adulthood. According to the DRI recommendations, adolescence is divided into two age groups: 9 through 13 years, and 14 through 18 years. Some of the important physiological changes that take place during this stage include the development of the primary sex characteristics (the reproductive organs), along with the onset of menstruation in females. This life stage is also characterized by the appearance of secondary sex characteristics, such as the growth of facial and body hair, the development of breasts in girls, the deepening of the voice in boys, and alterations in body proportions. All of these changes, as well as the accompanying mental and emotional adjustments, should be supported with sound nutrition.
The Onset of Puberty (Ages 9 through 13 years)
This period of physical development is divided into two phases. The first phase involves height increases from 20-25%. Puberty is second to the prenatal period in terms of rapid growth as the long bones stretch to their final, adult size. Girls typically grow 2 to 8 inches taller, while boys grow 4 to 12 inches taller. The second phase involves weight gain related to the development of bone, muscle, and fat tissue.
Energy and Macronutrients
The energy requirements for preteens differ according to biological sex, growth, and activity level. For ages 9 to 13, girls should consume about 1,400-2,200 kcal per day and boys should consume 1,600-2,600 kcal per day. Physically active preteens who regularly participate in sports or exercise need to eat a greater number of kcal to account for increased energy expenditures.
The AMDR recommendations remain 45-65% of total kcal from carbohydrates, 10-30% from protein, and 25-35% from fat. Foods that are high in fiber should make up the bulk of carbohydrate intake.
Micronutrients
Key vitamins needed during puberty include vitamins B12, D, and K. Adequate calcium intake is essential for building bone and preventing osteoporosis later in life. Young females need more iron beginning at the onset of menstruation, while young males need additional iron for the development of lean body mass. Almost all of these needs should be met with dietary choices, not supplements (although iron may be an exception). See Table 18.6.1 for specific recommended micronutrients amounts.
Late Adolescence (Ages 14 through 18 years)
After puberty, the rate of physical growth slows down. Girls stop growing taller around age 16, while boys continue to grow until ages 18-20. One of the psychological and emotional changes that takes place during this life stage includes the desire for independence as adolescents develop individual identities apart from their families. As teenagers make more and more of their own dietary decisions, parents or other caregivers and authority figures should guide them toward appropriate, nutritious choices. One way that teenagers assert their independence is by choosing what to eat. They often have their own money to purchase food and tend to eat more meals away from home. Older adolescents also can be curious and open to new ideas, which includes trying new kinds of food and experimenting with their diet. For example, teens will sometimes skip a main meal and snack instead. That is not necessarily problematic. Their choice of food is more important than the time or place.
However, too many poor choices can make young people nutritionally vulnerable. Teens should be discouraged from eating fast food, which has a high fat, sugar, and sodium content, or frequenting convenience stores and using vending machines, which typically offer poor nutritional selections. Other challenges that teens may face include obesity and eating disorders. At this life stage, young people still need guidance from parents and other caregivers about nutrition-related matters. It can be helpful to explain to young people how healthy eating habits can support activities they enjoy, such as skateboarding or dancing, or connect to their desires or interests, such as athletic performance or improved cognition.
As during puberty, growth and development during adolescence differs in males and females. Teenage girls experience a significant increase in body fat, while teenage boys often experience an increase in fat-free and skeletal mass, and a decrease in body fat.28 For both males and females, primary and secondary sex characteristics have fully developed and the rate of growth slows with the end of puberty.
Energy and Macronutrients
Adolescents have increased appetites due to increased nutritional requirements. Nutrient needs are greater in adolescence than at any other time in the life cycle, except during pregnancy. The energy requirements for ages 14 to 18 are 1,800-2,400 kcal for girls and 2,000-3,200 kcal for boys, depending on activity level. The extra energy required for physical development during the teenage years should be obtained from foods that provide nutrients instead of “empty calories.” Also, teens who participate in athletics must make sure to meet their increased energy needs.
Older adolescents are more responsible for their dietary choices than younger children, but parents and caregivers must make sure that teens continue to meet their nutrient needs. The AMDR for carbohydrates remains 45-65% of daily kcal and the adequate intake (AI) of fiber is 25-34 g per day (depending on daily kcal intake). Adolescents require more servings of grain than younger children, and should eat whole grains, such as wheat, oats, barley, and brown rice. The NAM recommends higher intakes of protein for growth in the adolescent population. The AMDR for protein remains 10-30% of daily kcal and lean proteins, such as meat, poultry, fish, beans, nuts, and seeds are excellent ways to meet those nutritional needs. The AMDR for fat remains 25-35% of daily kcal. It is also essential for young athletes and other physically active teens to intake enough fluids, because they are at a higher risk for becoming dehydrated.
Micronutrients
Micronutrient recommendations for adolescents are mostly the same as for adults, though children this age need more of certain minerals to promote bone growth (e.g., calcium and phosphorus, along with iron and zinc for girls). Again, vitamins and minerals should be obtained from food first, with supplementation for certain micronutrients only (such as iron).
The most important micronutrients for adolescents are calcium, vitamin D, vitamin A, and iron. Adequate calcium and vitamin D are essential for building bone mass. The recommendation for calcium is 1,300 mg for both boys and girls. Low-fat milk and cheeses are excellent sources of calcium and help young people avoid saturated fat and cholesterol. It can also be helpful for adolescents to consume products fortified with calcium, such as breakfast cereals and orange juice. Iron supports the growth of muscle and lean body mass. Adolescent girls also need to ensure sufficient iron intake as they start to menstruate. Girls ages 12 to 18 require 15 mg of iron per day. Increased amounts of vitamin C from orange juice and other sources can aid in iron absorption. Also, adequate fruit and vegetable intake allows for meeting vitamin A needs.
Table 18.6.1 Recommended Micronutrient Intakes during Adolescence
| Nutrient | Females, 14-18 Years | Males, 14-18 Years |
| Vitamin A (mcg) | 700.0 | 900.0 |
| Thiamin (mg) | 1.0 | 1.2 |
| Riboflavin (mg) | 1.0 | 1.3 |
| Niacin (mg) | 14 | 16 |
| Vitamin B6 (mg) | 1.2 | 1.3 |
| Folate (mcg) | 400.0 | 300.0 |
| Vitamin B12 (mcg) | 2.4 | 2.4 |
| Vitamin C (mg) | 65.0 | 75.0 |
| Vitamin D (mcg) | 15.0 | 15.0 |
| Vitamin E (mg) | 15.0 | 15.0 |
| Vitamin K (mcg) | 75.0 | 75.0 |
| Calcium (mg) | 1300.0 | 1300.0 |
| Iron (mg) | 15.0 | 11.0 |
| Magnesium (mg) | 360.0 | 410.0 |
| Phosphorus (mg) | 1250.0 | 1250.0 |
| Selenium (mcg) | 55.0 | 55.0 |
| Zinc (mg) | 9.0 | 11.0 |
18.7 Adulthood
Adulthood begins at the end of adolescence and continues until the end of one’s life.
Young Adulthood
Young adulthood is the period from ages 19 to 30 years. It is a stable time compared to childhood and adolescence. Physical growth has been completed and all of the organs and body systems are fully developed. Typically, a young adult who is active has reached his or her physical peak and is in prime health. During this life stage, it is important to continue to practice good nutrition. Healthy eating habits promote metabolic functioning, assist repair and regeneration, and prevent the development of chronic conditions. Proper nutrition and adequate physical activity at this stage not only promote wellness in the present, but also provide a solid foundation for the future.
With the onset of adulthood, good nutrition can help young adults enjoy an active lifestyle. The body of an adult does not need to devote its energy and resources to support the rapid growth and development that characterizes youth. However, the choices made during those formative years can have a lasting impact. Eating habits and preferences developed during childhood and adolescence influence health and fitness into adulthood. Some adults have gotten a healthy start and have established a sound diet and regular activity program, which helps them remain in good condition from young adulthood into their later years. Others carry childhood obesity into adulthood, which adversely affects their health. However, it is not too late to change course and develop healthier habits and lifestyle choices. Therefore, adults must monitor their dietary decisions and make sure their caloric intake provides the energy that they require, without going into excess.
Energy and Macronutrients
Young men typically have higher nutrient needs than young women. For ages 19-30, the energy requirements for women are 1,800-2,400 kcal, and 2,400-3,000 kcal for men, depending on activity level. These estimates do not include women who are pregnant or breastfeeding, who require a higher energy intake. For carbohydrates, the AMDR continues to be 45-65% of daily kcal. All adults, young and old, should eat fewer energy dense carbohydrates, especially refined, sugar dense sources, particularly for those who lead a more sedentary lifestyle. The AMDR for protein is 10-35% of total daily kcal, and should include a variety of lean meat and poultry, eggs, beans, peas, nuts, and seeds. The guidelines also recommend that adults eat at least two 4 oz servings of seafood per week.
It is also important to replace foods that are high in saturated fat with ones that are lower in solid fats and kcal. All adults should limit total fat to 20-35% of their daily kcal and keep saturated fatty acids to less than 10% of total kcal by replacing them with monounsaturated and polyunsaturated fatty acids. The adequate intake for fiber is 22-28 g per day for women and 28-34 g per day for men. Soluble fiber may help improve cholesterol and blood sugar levels, while insoluble fiber can help prevent constipation.
Micronutrients
Micronutrient needs in adults differ slightly according to sex. Young men and women who are very athletic and perspire a great deal may require extra sodium, potassium, and magnesium. Males require more of vitamins A, C, and K along with thiamin, riboflavin, and niacin. Females require extra iron due to menstruation. Therefore, it can be beneficial for some young adults to follow a daily multivitamin regimen to help meet nutrient needs. But as always, it is important to remember “food first, supplements second.”
Table 18.7.1 Recommended Micronutrient Intakes during Adulthood
| Nutrient | Females, 19+ Years | Males, 19+ Years |
| Vitamin A (mcg) | 700.0 | 900.0 |
| Thiamin (mg) | 1.1 | 1.2 |
| Riboflavin (mg) | 1.1 | 1.3 |
| Niacin (mg) | 14.0 | 16.0 |
| Vitamin B6 (mg) | 1.3 (19-50 yr) | 1.3 (19-50 yr) |
| 1.5 (51+ yr) | 1.7 (51+ yr) | |
| Folate (mcg) | 400.0 | 400.0 |
| Vitamin B12 (mcg) | 2.4 | 2.4 |
| Vitamin C (mg) | 75.0 | 90.0 |
| Vitamin D (mcg) | 15.0 (19-70 yr) | 15.0 (19-70 yr) |
| 20.0 (71+ yr) | 20.0 (71+ yr) | |
| Vitamin E (mg) | 15.0 | 15.0 |
| Vitamin K (mcg) | 90.0 | 120.0 |
| Calcium (mg) | 1000.0 (19-50 yr) | 1000.0 (19-70 yr) |
| 1200.0 (51+yr) | 1200.0 (71+ yr) | |
| Iron (mg) | 18.0 (19-50 yr) | 8.0 |
| 8.0 (51+ yr) | ||
| Magnesium (mg) | 310.0 (19-30 yr) | 400.0 (19-30 yr) |
| 320.0 (31+ yr) | 420.0 (31+ yr) | |
| Phosphorus (mg) | 700.0 | 700.0 |
| Selenium (mcg) | 55.0 | 55.0 |
| Zinc (mg) | 8.0 | 11.0 |
Middle Age
Middle age is defined as the period from age 31 to 50. The early period of this stage is very different from the end. For example, during the early years of middle age, many women experience pregnancy, childbirth, and lactation. In the latter part of this life stage, women face perimenopause, which is a transition period that leads up to menopause, or the end of menstruation. A number of physical changes take place in the middle-aged years, including the loss of bone mass in women due to dropping levels of estrogen during menopause. In both men and women, visual acuity declines, and by age 40 there can be a decreased ability to see objects at a close distance.29 All of these are signs of aging, as the human body begins to change in subtle and not-so-subtle ways. However, a middle aged person can remain vital, healthy, and near his or her physical peak with proper diet and adequate exercise.
During this stage of the human life cycle, adults begin to experience the first outward signs of aging. Wrinkles begin to appear, joints may ache after a highly active day, and body fat accumulates. There is also a loss of muscle tone and elasticity in the connective tissue.29 Many people in this stage may also notice a decline in endurance, the onset of wear-and-tear injuries (such as osteoarthritis), and changes in the digestive system. Wounds and other injuries may also take longer to heal. Body composition changes due to fat deposits in the trunk. To maintain health and wellness during the middle-aged years and beyond, it is important to:
- maintain a healthy body weight
- consume nutrient dense foods
- drink alcohol moderately or not at all
- avoid tobacco products
- engage in moderate aerobic physical activity at least 150 minutes per week
- engage in muscle strengthening activity at least two days per week
Energy and Macronutrients
The energy requirements for ages 31 to 50 are 1,800-2,200 kcal for women and 2,200-3,000 kcal for men, depending on activity level. These estimates do not include women who are pregnant or breastfeeding. Middle-aged adults must rely on healthy food sources to meet these needs. Following the dietary guidelines in the middle-aged years provides adequate but not excessive energy, vitamins, and minerals.
The recommended intake for carbohydrates, protein, fat, fiber, and fluids remain the same from young adulthood into middle age. It is important to avoid putting on excess weight and limiting intake of saturated fats and added sugars to help avoid cardiovascular disease, diabetes, and other chronic conditions.
Micronutrients
There are some differences, however, regarding micronutrients. For men, the recommendation for magnesium increases to 420 mg daily, while middle-aged women should increase their intake of magnesium to 320 mg per day. Other key vitamins needed during the middle-aged years include vitamins B6, B12 and folate to prevent elevation of homocysteine, a byproduct of metabolism that can damage arterial walls and lead to atherosclerosis, a cardiovascular condition.
Preventive/Defensive Nutrition
During the middle-aged years, preventive nutrition can promote wellness and help organ systems to function optimally throughout aging. Preventive nutrition is defined as dietary practices directed toward reducing disease and promoting health and well-being. Healthy eating in general, such as eating unrefined carbohydrates instead of refined carbohydrates and avoiding trans fats and saturated fats, helps to promote wellness. However, there are also some things that people can do to target specific concerns. One example is consuming foods high in antioxidants, such as strawberries, blueberries, and other colorful fruits and vegetables, to reduce risk of cancer. Omega-3 fatty acids can help to prevent coronary artery disease. These crucial nutrients are found in oily fish, including salmon, mackerel, tuna, herring, cod, and halibut. Other beneficial fats that are vital for healthy functioning include monounsaturated fats, which are found in plant oils, avocados, and pecans.
Menopause
In the middle-aged years, women undergo a specific change that has a major effect on their health. They begin the process of menopause, typically in their late 40s or early 50s. The ovaries slowly cease to produce estrogen and progesterone, which results in the end of menstruation. Menopausal symptoms can vary, but often include hot flashes, night sweats, and mood changes. The hormonal changes that occur during menopause can lead to a number of physiological changes as well, including alterations in body composition, such as weight gain in the abdominal area. Bone loss is another common condition related to menopause due to the loss of female reproductive hormones. When one loses a significant amount of bone, they likely have osteoporosis, increasing their risk of fractures, which can affect mobility and the ability to complete everyday tasks.30 See Chapter 15 for more information on osteoporosis.
Recommendations for women experiencing menopause or perimenopause (the stage just prior to the end of the menstruation) include31:
- consuming a variety of whole, nutrient dense foods like vegetables, fruits, whole grains, and lean protein sources such as beans and lentils
- avoiding caffeine, spicy foods, and alcohol to help prevent hot flashes
- eating foods rich in calcium, or taking physician prescribed calcium and vitamin D supplements
- reducing sodium intake
- being physically active at least 30 minutes at moderate intensity most days of the week, include strength training activities, and stretching to improve balance and flexibility and reduce the risk of falls and fractures
- drinking plenty of water
18.8 Older Age
The senior years are the period from age 51 until the end of life. A number of physiological and emotional changes take place during this life stage. For example, many older adults face serious health challenges, such as cancer, heart disease, diabetes, or dementia. Both men and women experience a loss of hormone production, muscle mass and strength, and undergo changes in body composition. Fat deposits build up in the abdominal area, which increases the risk for type 2 diabetes and cardiovascular disease. The skin becomes thinner and may take longer to heal after an injury. Also in the later years, the heart has to work harder because each pump is not as efficient as it used to be. Kidneys are not as effective in excreting metabolic products such as sodium and potassium, which can alter water balance and increase the risk for dehydration. In addition, immune function decreases and there is lower efficiency in the absorption of vitamins and minerals.
In addition, disorders of the nervous system can have profound effects. Dementia is the umbrella term for changes in the normal activity of the brain. Elderly adults who suffer from dementia may experience memory loss, agitation, and delusions. More than five million Americans have Alzheimer’s disease, the most common form of dementia. It is the sixth leading cause of death in the US.32 Neurological disorder and psychological conditions, such as depression, can influence attitudes toward food, along with the ability to prepare or ingest food. They might lead some adults to overindulge to compensate for stress or emotions that are difficult to handle. Other adults might eat less or pay less attention to their diet and nutritional needs. Older adults may also need guidance from dietitians and healthcare professionals to make the best dietary choices for this stage of life.
In older age, blood pressure rises and the immune system may have more difficulty battling invaders and infections. The skin becomes more wrinkled and hair has turned gray or white or fallen out, resulting in hair thinning. Older adults may gradually lose an inch or two in height. Also, short-term memory might not be as keen as it once was.
Being either underweight or overweight is a major concern for the elderly. However, many older adults remain in relatively good health and continue to be active into their golden years. Good nutrition is often the key to maintaining health later in life. In addition, the fitness and nutritional choices made earlier in life set the stage for continued health and happiness. Older adults should continue to consume nutrient dense foods and remain physically active. However, deficiencies are more common after age 60, primarily due to reduced intake or absorption. The loss of mobility among frail, home-bound elderly adults also impacts their access to healthy, diverse foods.
Energy and Macronutrients
Due to reductions in lean body mass and metabolic rate, older adults require less energy than younger adults. The energy requirements for people ages 51 and over are 1,600-2,200 kcal for women and 2,000-2,800 kcal for men, depending on activity level. The decrease in physical activity that is typical of older adults also influences nutritional requirements. The AMDRs for carbohydrates, protein, and fat remain the same from middle age into old age. However, it is recommended that the elderly consume 1.2-2.0 g of protein per kg body weight to help prevent significant muscle loss.33 Older adults should choose more unrefined carbohydrates such as whole grains and brown rice instead of refined grains. Fiber is especially important in preventing constipation and diverticulitis, and may also reduce the risk of colon cancer. Protein should be lean and healthy fats, such as omega-3 fatty acids, are part of any good diet.
Micronutrients
An increase in certain micronutrients can help maintain health during this life stage. The recommendations for calcium increase to 1,200 mg per day for women beginning at age 51 and men at age 71 to slow bone loss. Also to help protect bones, vitamin D recommendations increase from 15 to 20 mcg per day for men and women. Vitamin B6 recommendations rise to 1.7 mg per day for older men and 1.5 mg per day for older women to help lower levels of homocysteine and protect against cardiovascular disease. For elderly women, higher iron levels are no longer needed postmenopause and recommendations decrease to 8 mg per day. People over age 50 should eat foods rich with all of these micronutrients.
Nutritional Concerns for Older Adults
Dietary choices can help improve health during this life stage and address some of the nutritional concerns that many older adults face. In addition, there are specific concerns related to nutrition that affect adults in their later years. They include medical problems, such as disability and disease, which can impact diet and activity level. For example, dental problems can lead to difficulties with chewing and swallowing, which in turn can make it hard to maintain a healthy diet. The use of dentures or the preparation of chopped or pureed foods can help solve this problem. There also is a decreased thirst response in the elderly, and the kidneys have a decreased ability to concentrate urine, both of which can lead to dehydration.
Sensory Issues
At about age 60, taste buds begin to decrease in size and number. As a result, the taste threshold is higher in older adults, meaning that more of the same flavor must be present to detect the taste. Many elderly people lose the ability to distinguish between salty, sour, sweet, and bitter flavors. This can make food seem less appealing and decrease the appetite. An intake of foods high in sugar and sodium can increase due to an inability to discern those tastes. The sense of smell also decreases, which impacts attitudes toward food. Sensory issues may also affect the digestion because the taste and smell of food stimulates the secretion of digestive enzymes in the mouth, stomach, and pancreas.
Gastrointestinal Issues
A number of gastrointestinal issues can affect food intake and digestion among the elderly. Saliva production decreases with age, which affects chewing, swallowing, and taste. Other digestive secretions decline later in life as well, which can lead to atrophic gastritis (inflammation of the lining of the stomach). This interferes with the absorption of some vitamins and minerals. Reduction of the digestive enzyme lactase results in a decreased tolerance for dairy products. Slower gastrointestinal motility can result in more constipation, gas, and bloating, and can also be tied to low fluid intake, decreased physical activity, and a diet low in fiber, fruits, and vegetables.
Dysphagia
Some older adults have difficulty getting adequate nutrition because of the disorder dysphagia, which impairs the ability to swallow. Any damage to the parts of the brain that control swallowing can result in dysphagia, therefore having a cerebrovascular accident, more commonly called a stroke, is a common cause. Dysphagia is also associated with advanced dementia because of overall brain function impairment. To assist older adults suffering from dysphagia, it can be helpful to alter food consistency. For example, solid foods can be chopped, ground, or pureed to allow a more successful and safe swallow. This decreases the risk of aspiration, which occurs when food enters the respiratory tract and can result in pneumonia. Typically, speech therapists, physicians, and dietitians work together to determine the appropriate diet for dysphagia patients.
Vision Problems
Many older people suffer from vision problems and a loss of vision. Age-related macular degeneration is the leading cause of blindness in Americans over age 60.34 This disorder can make food planning and preparation extremely difficult and people who suffer from it often must depend on caregivers for their meals. Self-feeding may be difficult if an elderly person cannot see his or her food clearly. Friends and family members can help older adults with shopping and cooking. Food-assistance programs for older adults (such as Meals on Wheels) can also be helpful.
Diet may help to prevent macular degeneration. Consuming colorful fruits and vegetables increases the intake of lutein and zeaxanthin. Several studies have shown that these antioxidants provide protection for the eyes. Lutein and zeaxanthin are found in green, leafy vegetables such as spinach, kale, and collard greens, and also corn, peaches, squash, broccoli, Brussels sprouts, orange juice, and honeydew melon.35
Obesity in Old Age
Similar to other life stages, obesity is a concern for the elderly. Adults over age 60 are more likely to be obese than young or middle-aged adults. As explained previously, excess body weight has severe consequences. Being overweight or obese increases the risk for potentially fatal conditions that can afflict the elderly. They include cardiovascular disease, which is the leading cause of death in the US and type 2 diabetes, the seventh leading cause of death in the US annually.
For older adults who are overweight or obese, dietary changes to promote weight loss should be combined with an exercise program to protect muscle mass. This is because dieting reduces muscle as well as fat, which can exacerbate the loss of muscle mass due to aging. Although weight loss among the elderly can be beneficial, it is best to be cautious and consult with a healthcare professional before beginning a weight loss program.
The Anorexia of Aging
In addition to concerns about obesity among senior citizens, being underweight can be a major problem. A condition known as the anorexia of aging is characterized by poor food intake, which results in dangerous weight loss. This major health problem among the elderly leads to a higher risk for immune deficiency, frequent falls, muscle loss, and cognitive deficits. Reduced muscle mass (sarcopenia) and physical activity mean that older adults need fewer kcal per day to maintain a normal weight. It is important for health care providers to examine the causes for anorexia of aging among their patients, which can vary from one individual to another. Understanding why some elderly people eat less as they age can help healthcare professionals assess the risk factors associated with this condition. Decreased intake may be due to disability or the lack of a motivation to eat. Also, many older adults skip at least one meal each day, sometimes because of financial reasons. As a result, some elderly people are unable to meet even reduced energy needs.
Nutritional interventions should focus primarily on a healthy diet. Remedies can include increasing the frequency of meals and adding healthy, high-calorie foods (such as nuts, potatoes, whole-grain pasta, and avocados) to the diet. Liquid supplements between meals may help to improve caloric intake. Health care professionals should consider a patient’s habits and preferences when developing a nutritional treatment plan. After a plan is in place, patients should be weighed on a weekly basis until they show improvement.
Longevity and Nutrition
The foods you consume in your younger years influence your health as you age. Good nutrition and regular physical activity can help you live longer and healthier. Conversely, poor nutrition and a lack of exercise can shorten your life and lead to medical problems. The right foods provide numerous benefits at every stage of life. They help an infant grow, an adolescent develop mentally and physically, a young adult achieve his or her physical peak, and an older adult cope with aging. Nutritious foods form the foundation of a healthy life at every age.
Key Takeaways
- Starting BMI determines how much weight a woman needs to gain throughout her pregnancy. In an average pregnancy, a woman gains an extra 30 lb.
- During the second and third trimesters, a woman’s energy requirements increase by 340 kcal per day for the second trimester and 450 kcal per day for the third trimester. For the first six months of life, children should consume breast milk exclusively.
- For the next six months, solid foods should be introduced gradually into an infant’s diet as parents and caregivers continue to provide breast milk.
- Breast milk is ideal for infants and provides all of the nutrients they need to grow and develop. Breastfeeding provides numerous benefits for both a mother and her infant.
- By the toddler years, young children are able to self-feed and begin to develop eating habits and preferences.
- Some food- and nutrition-related problems that can occur during the toddler years include choking, picky eating and food jags, early childhood caries, and iron deficiency anemia.
- The recommended intakes of macronutrients and micronutrients for children are higher relative to body size compared with nutrient needs during adulthood. Children’s daily energy needs vary depending on their level of physical activity.
- Beginning in adolescence, some micronutrient needs begin to differ by biological sex.
- Nutritional concerns for middle-aged adults relate to menopause and the prevention of chronic disease.
- Older adults are more susceptible to medical problems, such as disability and disease, which can impact appetite, the ability to plan and prepare food, chewing and swallowing, self-feeding, and general nutrient intake.
Portions of this chapter were taken from OER Sources listed below:
Tharalson, J. (2019). Nutri300:Nutrition. https://med.libretexts.org/Courses/Sacremento_City_College/SSC%3A_Nutri_300_(Tharalson)
Titchenal, A., Calabrese, A., Gibby, C., Revilla, M.K.F., & Meinke, W. (2018). Human Nutrition. University of Hawai'i at Manoa Food Science and Human Nutrition Program Open Textbook. https://pressbooks.oer.hawaii.edu
Additional References:
- Centers for Disease Control and Prevention. (2020, February 26). Before pregnancy. Information for men. https://www.cdc.gov/preconception/men.html
- Jarlenski, M. P., Bennett, W. L., Bleich, S. H., Barry, C. L., & Stuart, E. A. (2014). Effects of breastfeeding on postpartum weight loss among US women. Preventive Medicine, 69, 146-50. https://doi:10.1016/j.ypmed.2014.09.018
- Most, J., Dervis, S., Haman, F., Adamo, K. B., & Redman, L. M. (2019). Energy intake requirements in pregnancy. Nutrients, 11(8), 1812. https://doi:10.3390/nu/11081812
- Office on Women’s Health. (2019, March 14). Staying Healthy and Safe. United States Department of Health and Human Services.https://www.womenshealth.gov/pregnancy/youre-pregnant-now-what/staying-healthy-and-safe/#1
- American College of Obstetricians and Gynecologists. (2010). Moderate caffeine consumption during pregnancy. Committee Opinion No. 462. Obstetrics & Gynecology 116, 467-8. https://www.acog.org/clinical/clinical-guidance/committee-opinion/articles/2010/08/moderate-caffeine-consumption-during-pregnancy
- Centers for Disease Control and Prevention. (2016, December 16). Listeria (listeriosis). https://www.cdc.gov/listeria/risk-groups/pregnant-women.html
- Lumish, R. A., Young, S. L., Lee, S., Cooper, E., Presman, E., Guillet, R., & O’Brien, K. O. (2014). Gestation iron deficiency is associated with pica behavior in adolescents. The Journal of Nutrition, 144(10), 1533-1539. doi:10.3945/jn.114.192070.
- Zhou, T., Sun, D., Li, X., Heianza, Y., Nisa, H., Hu, G., Pei, X., Shang, X., & Qi, L. (2018). Prevalence and trends in gestational diabetes mellitus among women in the United States, 2006-2016. Diabetes, 67(Suppl1). https://doi:10.2237/db18-121-OR
- American Pregnancy Association. (n.d.). Breastfeeding vs bottle feeding formula. https://americanpregnancy.org/breastfeeding/breastfeeding-vs-bottle-feeding-formula/
- Centers for Disease Control and Prevention. (2019, December 31). Breastfeeding report card, United States 2018. https://www.cdc.gov/breastfeeding/data/reportcard.htm
- World Health Organization (2020. April 1). Infant and young children feeding: Key facts. https://www.who.int/news-room/fact-sheets/detail/infant-and-young-child-feeding
- United States Department of Health and Human Services. (2011, January 20). Executive summary: The Surgeon General’s call to action to support breastfeeding. Office of the Surgeon General. https://www.hhs.gov/sites/default/files/breastfeeding-call-to-action-executive-summary.pdf
- Pillay, J., & Davis, T. J. (2020, April 27). Physiology, lactation. StatPearls. https://www.ncbi.nlm.nih.gov/books/NBK499981/
- Ballard, O., & Morrow, A. L. (2013). Human milk composition: Nutrients and bioactive factors. Pediatric Clinics of North America, 60(1), 49-74. https://doi:10.1016.j.pcl.2012.10.002
- American Pregnancy Association. (2020, June, 25). Breastfeeding: Overview. http://www.americanpregnancy.org/firstyearoflife/breastfeedingoverview.htm.
- Centers for Disease Control and Prevention. (2019, December 28). Alcohol. https://www.cdc.gov/breastfeeding/breastfeeding-special-circumstances/vaccinations-medications-drugs/alcohol.html
- Bravi, F., Wiens, F., Decarli, A., Dal Pont, A., Agostoni, C., & Ferraroni, M. (2016). Impact of maternal nutrition on breast-milk composition: a systematic review. The American Journal of Clinical Nutrition, 104(3), 646-662. https://doi:10.3945/ajcn.115.120881.
- McMillan, B. (2008). Illustrated atlas of the human body. Weldon Owen.
- Centers for Disease Control and Prevention. (2019, December 19). Vitamin K deficiency bleeding. https://www.cdc.gov/ncbddd/vitamink/faqs.html
- Centers for Disease Control and Prevention. (2019, October 17). When, what, and how to introduce solid foods. https://www.cdc.gov/nutrition/infantandtoddlernutrition/foods-and-drinks/when-to-introduce-solid-foods.html
- United States Department of Agriculture. (2016, October). Healthy eating for preschoolers. ChooseMyPlate. https://choosemyplate-prod.azureedge.net/sites/default/files/tentips/healthy_eating_for_preschoolers.pdf)
- The Ellyn Satter Institute. (n.d.). Division of responsibility in feeding. https://www.ellynsatterinstitute.org/how-to-feed/the-division-of-responsibility-in-feeding/
- World Health Organization. (2019, September 3). Facts and figures on childhood obesity. https://www.who.int/end-childhood-obesity/facts/en/
- Fryar, C. D., Carroll, M. D., & Ogden, C. L. (2014). Prevalence of overweight and obesity among children and adolescents: United States, 1963-1965 through 2011-2012. National Center for Health Statistics. https://www.cdc.gov/nchs/data/hestat/obesity_child_11_12/obesity_child_11_12.pdf
- Hales, C. M., Carroll, M. D., Fryar, C. D., & Ogden, C. L. (2017). Prevalence of obesity among adults and youth: 2015-2016. National Center for Health Statistics. Data Brief, no 288. https://www.cdc.gov/nchs/products/databriefs/db288.htm
- Ervin, R. B., Kit, B. K., Carroll, M. D., & Ogden, C. L. (2012, February). Consumption of added sugar among US Children and Adolescents, 2005-2008. National Center for Health Statistics. Data Brief, no. 87. https://www.cdc.gov/nchs/products/databriefs/db87.htm
- Gillman, M. W., Rifas-Shiman, S. L., Frazier, L., Rockett, H. R., Camargo, C. A., Field, A. E., Berkey, C. S., & Colditz, G. A. (2000). Family dinner and diet quality among older children and adolescents. Archives of Family Medicine 9, 235-240.
- Loomba-Albrecht, L.A., & Styne, D. M. (2009). Effect of puberty on body composition. Current Opinion in Endocrinology, Diabetes and Obesity, 16(1), 10-15. https://doi:10.3945/ajcn.115.120881
- Poland, E.U., & Taylor, D.R. (2003). Journey across the lifespan: Human development and health promotion. Davis Company.
- National Osteoporosis Foundation. (n.d.). What is osteoporosis and what causes it? https://www.nof.org/patients/what-is-osteoporosis/
- Wolfram, T. (2019). Eating right during menopause. Academy of Nutrition and Dietetics. https://www.eatright.org/health/wellness/healthy-aging/eating-right-during-menopause
- Alzheimer’s Association. (n.d.). Facts and Figures. https://www.alz.org/alzheimers-dementia/facts-figures
- Baum, J.I.,Kim, I-Y., & Wolfe, R.R. (2016). Protein consumption and the elderly. Nutrients, 8(6), 359. doi:10.3390%2Fnu8060359
- National Eye Institute. (2019. July 17). Age-related macular degeneration (AMD) data and statistics. National Institutes of Health. https://www.nei.nih.gov/learn-about-eye-health/resources-for-health-educators/eye-health-data-and-statistics/age-related-macular-degeneration-amd-data-and-statistics
- Eisenhauer, B., Natoli, S., Liew, G., & Flood, V. M. (2017). Lutein and zeaxanthin-food sources, bioavailability and dietary variety in age-related macular degeneration protection. Nutrients, 9(2), 120. https://doi.org/10.3390/nu9020120
very small finger-like projections on the tips of the villi of the small intestine
macronutrients that can provide energy in the form of kilocalories (kcal)
chemical energy obtained from the breakdown of food molecules and released to fuel cellular processes
unit of measurement of food energy; the amount of energy required to raise 1 kilogram of water 1 degree Celsius.
one thousand calories, denoted as kcal or Calorie (capital C) on nutrition food labels
term used in chemistry to denote that a molecule contains the carbon atom
main form of carbohydrate in the body
stored form of glucose in animals including humans; stored in liver and skeletal muscle
stored form of carbohydrate in plants
building blocks of protein
the amount of nutrients a food contains relative to the energy it provides
Food or beverages such as sugary sodas or candy containing calories but no beneficial nutrients
non-nutritive chemical compounds found in the edible parts of plants that provide characteristics to the plant like color, taste, smell. They may also provide health benefits beyond the traditional nutrients
muscular rings separating digestive organs that open and close to allow food to move through the digestive tract in a more orderly fashion
types of scientific studies that observe what happens in a population in relation to health over time in order to find risk factors for a health event; these types of studies do not determine cause
studies that change one variable between groups to determine causal relationships
a type of research study design in which neither the participant nor the researcher know in which group (treatment or control) the participant is assigned; It is a way to minimize bias
a substance that has no therapeutic effect
group in a research study that does not receive any type of treatment
letter used in research studies to indicate the number of participants in the study; ex. n=150 means there are 150 participants in the study. Generally the higher the n the more credible the results of the study
factors other than the ones being tested in a research study that could be influencing the results. It is important to control for as many variables as possible to assure research results are valid
