Since the 1980s, the prevalence of obesity (defined as BMI of 30 or greater) in the United States has increased dramatically. Data collected by the Centers for Disease Control and Prevention show rising rates of obesity across the nation, state-by-state.1Fig 7.17. Each year since 1990, the CDC has published maps of the United States in which states are color-coded based on the percentage of their population estimated to be obese. The maps show a clear increase in the prevalence of obesity between 1990 and 2010.

The methods used by the CDC to collect the data changed in 2011, so we can’t make direct comparisons between the periods before and after that change, but the trend has continued. Every year, more and more people in the U.S. report having a BMI that classifies them as having obesity, a trend that public health officials have labeled the obesity epidemic.Fig 7.18. The prevalence of obesity among U.S. adults has continued to rise between 2011 and 2020.


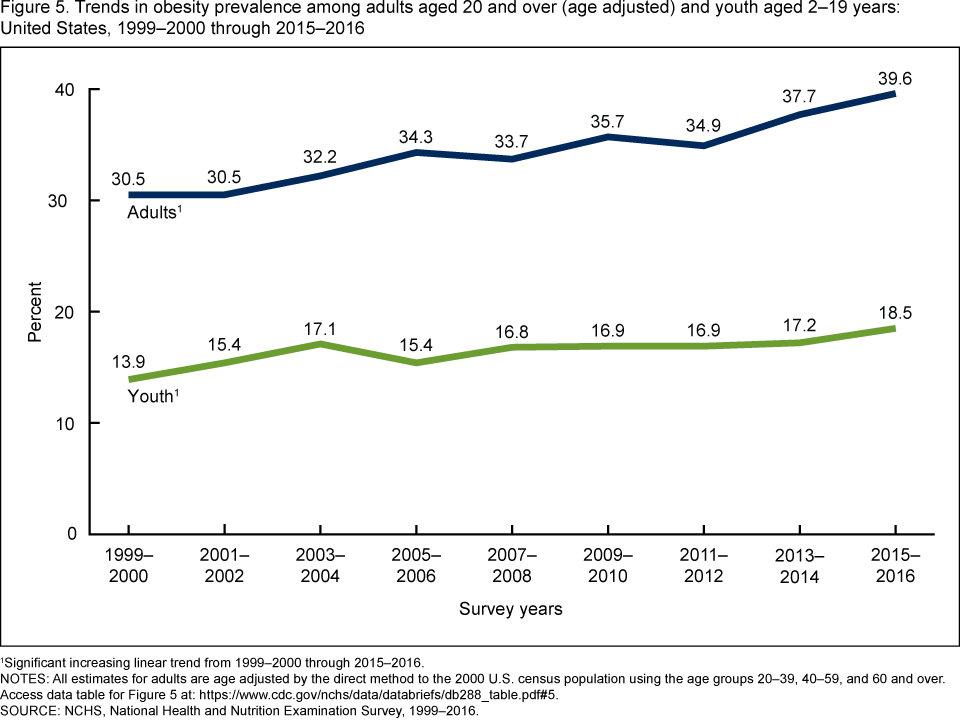
These trends are unmistakable, and they’re not just occurring in adults. Childhood obesity has seen similar increases over the last few decades. This is a concern because the metabolic and health effects of carrying too much weight can be compounded over a person’s lifetime, and people with obesity in childhood are more likely to also have obesity as adults.2
Fig 7.19. Between 1999 and 2016, the prevalence of obesity in both children and adults has risen steadily.

While obesity is a problem across the United States, it affects some groups of people more than others. Based on 2017-2018 data, the prevalence of obesity is 50 percent among Black adults, 45 percent among Hispanic adults, 42 percent among white adults, and 17 percent among Asian adults in the U.S. Overall, people who are college-educated and have a higher income are less likely to be obese.3 These health disparities point to the importance of looking at social determinants of health when examining causes and solutions. Not everyone has the same opportunity for good health, or an equal ability to make changes to their circumstances, because of factors like poverty and longstanding inequities in how resources are invested in communities.4
In addition to the health issues that can be associated with obesity, excess weight is also associated with greater costs of medical care. Cost estimates vary widely, in part because it’s very difficult to tease out health issues caused by obesity versus those correlated with it. A 2016 review of studies found that, on average, a person with obesity had $1,901 greater medical costs than a person classified as normal weight, adding up to $149 billion in the United States.5 A 2021 study reported similar cost estimates.6 The obesity epidemic is also not unique to the United States. Obesity is rising around the globe, and in 2015, it was estimated to affect 2 billion people worldwide, making it one of the largest factors affecting poor health in most countries.7 Previously, overweight and obesity mainly affected high-income countries, but some of the most dramatic increases in childhood overweight over the last decade have been in low income countries, such as those in Africa and South Asia.
Despite the gravity of the problem, no country has yet been able to implement policies that have reversed the trend and brought about a decrease in obesity. This represents “one of the biggest population health failures of our time,” wrote an international group of researchers in the journal The Lancet in 2019.9 Turning the tide will require an understanding of the complex causes of the rise in excess weight. As we’ll see, these are interwoven into our environments, economies, societies, and policies, and we can thus assume that effective solutions will need to go far beyond the simplistic advice that people should “eat less and move more.”
Possible Causes of Excess Weight
What has caused the rise in obesity around the world? This question is still an active area of debate among researchers. The predominant explanation comes back to the concept of energy balance: A chronic shift towards positive energy balance—consuming more energy or calories than expended—has led to a gradual but persistent increase in body weight. This shift is thought to be the result of changes in the environments in which we live, which include fewer opportunities for physical activity and greater availability and marketing of inexpensive, convenient, energy-dense foods.10
Putting the focus on energy balance often leads people to assume that obesity is an individual problem—that those who weigh more simply need to change their behavior to eat less and exercise more, and if this doesn’t work, it must be because of a personal failing, such as a lack of self-control or motivation. However, science tells us that the reality is far more complex. Many factors can contribute to energy balance, and neurological and hormonal control of food intake and energy expenditure mean that it’s difficult to maintain a negative energy balance and weight loss. Some researchers also argue that food intake and physical activity can’t explain the continued increase in body weight, and we need to look to alternative explanations.11 In the sections below, we discuss some of the hypothesized causes for the rise in obesity, acknowledging there are likely multiple causes to this complex issue.
Environment and Physical Activity
Many of us live in what researchers and public health experts call “obesogenic environments.” That is, the ways in which our neighborhoods are built and our lives are structured influence our physical activity and food intake to encourage weight gain.12 Human physiology and metabolism evolved in a world where obtaining enough food for survival required significant energy investment in hunting or gathering—very different from today’s world where more people earn their living in sedentary occupations. From household chores, to workplace productivity, to daily transportation, getting things done requires fewer calories than it did in past generations.
Fig 7.20. Some elements of our environment that may make it easier to gain weight include sedentary jobs, easy access to inexpensive calories, and cities built more for car travel than for physical activity.

Our jobs have become more and more sedentary, with fewer opportunities for non-exercise thermogenesis (NEAT) throughout the day. There’s less time in the school day for recess and physical activity, and lack of neighborhood safety can limit kids’ ability to get out and play after the school day is over. Our towns and cities are built more for cars than for walking or biking. We can’t turn back the clock on human progress, and finding ways to stay active in modern environments is a significant challenge.
That said, recent research has called into question the role of physical activity in driving the rise in obesity. Studies of modern hunter-gatherer societies on the savannas of Africa have found that these very active people burn a similar number of calories each day as adults living more sedentary lifestyles in modern cities.13 In addition, even as rates of obesity have continued to increase, research suggests that physical activity among U.S. adults has also been increasing.11 Also, some studies find that people with higher BMI are more physically active than those in the normal weight category. “These findings contrast with conventional views that primarily attribute the cause of obesity to sedentary lifestyles and suggest that compensatory metabolic adaptations maintain total energy expenditure relatively constant among human populations and across various levels of physical activities,” write the authors of the Joint International Consensus Statement for Ending Stigma of Obesity.14 Being physically active benefits our health in a multitude of ways, including preventing chronic diseases often associated with higher body weight, but it’s not clear how much moving more affects long term energy balance or weight.
VIDEO: This short video explains some of the research on NEAT and efforts to increase it in our lives. James Levine: ‘I Came Alive as a Person’ (3 min), NOVA’s Secret Life of Scientists and Engineers, https://youtu.be/fLgGf0BO4tw.
Food Intake and Diet Quality
Our environments can also impact our food choices. We’re surrounded by vending machines, fast food restaurants, coffeeshops, and convenience stores that offer quick and inexpensive access to calories. These foods are also heavily advertised, and especially when people are stretched thin by working long hours or multiple jobs, they can be a welcome convenience. However, they tend to be more calorie-dense (and less nutrient-dense) and more heavily processed compared with home-cooked food. In addition, portion sizes at restaurants, especially fast food chains, have increased over the decades, and people are eating at restaurants more and cooking at home less. A randomized controlled trial found that participants had a greater caloric intake when eating processed foods compared with unprocessed foods, and eating more fruits and vegetables and less processed foods has been shown to be associated with less weight gain over time.10,15
Social Determinants of Health
As mentioned earlier in this unit, social determinants of health are the conditions in the places where people live, learn, work, and play that can affect health. They include factors related to socioeconomic instability, education, healthcare access and quality, neighborhood and built environment, and social and community context.4 In the United States, people with more disadvantaged social determinants of health have a greater incidence of obesity, emphasizing the importance of addressing systemic inequities to improve health of all Americans.16
Social determinants such as poverty and socioeconomic instability decrease opportunities for health in many ways. People living in poorer neighborhoods often lack grocery stores where they can purchase fresh fruits and vegetables and basic ingredients for cooking at home. Such areas are called food deserts—where healthy foods simply aren’t available or easily accessible. In these neighborhoods, people rely more on packaged and convenience foods that are more highly processed and may lead to greater energy intake.
People living with lower and less stable incomes also have to contend with food insecurity. Food security means “access by all people at all times to enough food for an active, healthy life.”16 Food insecurity means an inability to consistently obtain adequate food. It may seem counter-intuitive, but in the United States, food insecurity is linked to obesity. That is, people who have difficulty obtaining enough food are more likely to become obese and to suffer from diabetes and hypertension. This is likely related to the fact that inexpensive foods tend to be high in calories but low in nutrients, and when these foods form the foundation of a person’s diet, they can cause both obesity and nutrient deficiencies. It’s estimated that 12 percent of U.S. households are food insecure, and food insecurity is higher among Black (22 percent) and Latino (18 percent) households.17
Poor neighborhoods are also sometimes not safe or pleasant places to walk, play, or exercise. They may have busy traffic and polluted air, and they may lack sidewalks, green spaces, and playgrounds. A person living in this type of neighborhood will find it much more challenging to incorporate physical activity into their day compared with someone living in a neighborhood where it’s safe to walk to school or work, play at a park, ride a bike, or go for a run.
Social determinants of health likely drive and compound the racial and ethnic differences in obesity prevalence. Studies show that U.S. regions with more racial inequality in poverty, unemployment, and homeownership—all factors driven by historic and present-day inequities—have greater rates of obesity. In addition, experiencing racism and bias results in chronic stress, which is associated with greater weight gain.18-19

Figure 7.21. Social and economic inequities result in accumulated conditions that can increase risk of obesity and other health conditions.19
Genetics
What about genetics? While it’s true that our genes can influence our susceptibility to weight gain, researchers say genes can’t be the sole cause of the increasing prevalence of obesity. Genes take many generations to evolve, and the rise in obesity has occurred over just the last 40 to 50 years—only a few generations. When our grandparents were children, they were much less likely to become obese than our own children. That’s not because their genes were different, but more likely because they grew up in different conditions. However, it is true that a person’s genes can influence their susceptibility to weight gain in this environment, and obesity is more prevalent in some families. Research shows that about 50 to 75 percent of the variation in BMI is explained by genetic makeup.10
Dieting and Weight Stigma
We live in a society saturated by diet culture: Beliefs continuously promoted by diet companies, media, and influencers that center the idea that being thin is the same as being healthy, and that anyone who applies themselves by eating the right foods in the right amounts can achieve that ideal. But ironically, diet culture may contribute to weight gain. Studies show that dieting during adolescence is associated with greater risk of becoming overweight and of developing an eating disorder.20 Having a greater “drive for thinness” in adolescence is associated with similar attitudes and weight gain in adulthood.21 There’s also some research that finds that experiencing cycles of weight loss and weight regain (i.e., weight cycling or “yo-yo dieting”) may cause people to gain even more weight over time, although the evidence on this point is somewhat mixed and controversial.22,23
In addition, living in a larger body and experiencing weight stigma, which has been shown to affect people at home, in social settings, in the workplace, and in healthcare settings, may also contribute to weight gain. Experiencing weight stigma is associated with greater stress, less access to healthcare, less physical activity, and greater weight gain.24
Other Possible Causes
Many other possible causes of weight gain have been investigated and likely contribute on some level to the increasing prevalence of obesity:
- Many medications that may improve our health are also known to cause weight gain. These include some medications used to treat common conditions such as diabetes, hypertension, autoimmune disorders, and depression.14
- Greater exposure to endocrine disrupting chemicals, such as those found in food packaging and pollutants, is associated with weight gain.14
- Not getting enough sleep or being under greater stress is associated with weight gain.
- Changes in the gut microbiome (the bacteria living in our gastrointestinal tract), caused by changing dietary patterns and environmental exposures to microbes, may predispose people to weight gain.11
- Having had adverse childhood experiences (ACEs), defined as intensive stressors and traumatic events occuring in the first 18 years of life, is associated with a greater risk of obesity in adolescence and adulthood. ACEs include “recurring childhood maltreatment (physical, emotional and sexual abuse, and neglect), household dysfunction (witnessing violence between parents or caregivers, parental separation, incarceration or substance abuse of a household member, mental illness, and attempted or complete suicide by a family member), and community violence that deprive the sense of stability, safety and development of a child.” Experiencing ACEs can cause changes in the brain, hormone levels, inflammation, sleep quality, and immune function, all of which can affect a person’s risk of developing obesity.25
some of the causes and potential solutions for obesity. The Weight of the Nation: Poverty and Obesity (24 min) https://youtu.be/7MJnm5X9NN0 and The Weight of the Nation: Healthy Foods and Obesity Prevention (31 min)
Self-Check:
References:
- 1(CDC). (2021, September 27). Adult Obesity Prevalence Maps. Retrieved May 13, 2022, from Centers for Disease Control and Prevention website: https://www.cdc.gov/obesity/data/prevalence-maps.html
- 2Golden, N. H., Schneider, M., Wood, C., Committee on Nutrition, Committee on Adolescence, & Section on Obesity. (2016). Preventing Obesity and Eating Disorders in Adolescents. Pediatrics, 138(3), e20161649. https://doi.org/10.1542/peds.2016-1649
- 3CDC. (2021, September 30). Adult Obesity Facts | Overweight & Obesity | CDC. Retrieved May 13, 2022, from https://www.cdc.gov/obesity/data/adult.html
- 4Trust for America’s Health. (2021). The State of Obesity: Better Policies for a Healthier America. Retrieved from https://www.tfah.org/wp-content/uploads/2021/09/2021ObesityReport_Fnl.pdf
- 5Kim, D. D., & Basu, A. (2016). Estimating the Medical Care Costs of Obesity in the United States: Systematic Review, Meta-Analysis, and Empirical Analysis. Value in Health: The Journal of the International Society for Pharmacoeconomics and Outcomes Research, 19(5), 602–613. https://doi.org/10.1016/j.jval.2016.02.008https://doi.org/10.1016/j.jval.2016.02.008
- 6Ward, Z. J., Bleich, S. N., Long, M. W., & Gortmaker, S. L. (2021). Association of body mass index with health care expenditures in the United States by age and sex. PloS One, 16(3), e0247307. https://doi.org/10.1371/journal.pone.0247307
- 7Swinburn, B. A., Kraak, V. I., Allender, S., Atkins, V. J., Baker, P. I., Bogard, J. R., … Dietz, W. H. (2019). The Global Syndemic of Obesity, Undernutrition, and Climate Change: The Lancet Commission report. The Lancet, 393(10173), 791–846. https://doi.org/10.1016/S0140-6736(18)32822-8
- 8UNICEF. (2019). The State of the World’s Children 2019. Children, Food and Nutrition: Growing well in a changing world. New York.
- 9Jaacks, L. M., Vandevijvere, S., Pan, A., McGowan, C. J., Wallace, C., Imamura, F., … Ezzati, M. (2019). The obesity transition: Stages of the global epidemic. The Lancet Diabetes & Endocrinology, 7(3), 231–240. https://doi.org/10.1016/S2213-8587(19)30026-9
- 10Hall, K. D., Farooqi, I. S., Friedman, J. M., Klein, S., Loos, R. J. F., Mangelsdorf, D. J., O’Rahilly, S., Ravussin, E., Redman, L. M., Ryan, D. H., Speakman, J. R., & Tobias, D. K. (2022). The energy balance model of obesity: Beyond calories in, calories out. The American Journal of Clinical Nutrition, 115(5), 1243–1254. https://doi.org/10.1093/ajcn/nqac031
- 11Mozaffarian, D. (2022). Perspective: Obesity—an unexplained epidemic. The American Journal of Clinical Nutrition, 115(6), 1445–1450. https://doi.org/10.1093/ajcn/nqac075
- 12Townshend, T., & Lake, A. (2017). Obesogenic environments: Current evidence of the built and food environments. Perspectives in Public Health, 137(1), 38–44. https://doi.org/10.1177/1757913916679860
- 13Pontzer, H., Raichlen, D. A., Wood, B. M., Mabulla, A. Z. P., Racette, S. B., & Marlowe, F. W. (2012). Hunter-Gatherer Energetics and Human Obesity. PLOS ONE, 7(7), e40503. https://doi.org/10.1371/journal.pone.0040503
- 14Rubino, F., Puhl, R. M., Cummings, D. E., Eckel, R. H., Ryan, D. H., Mechanick, J. I., Nadglowski, J., Ramos Salas, X., Schauer, P. R., Twenefour, D., Apovian, C. M., Aronne, L. J., Batterham, R. L., Berthoud, H. R., Boza, C., Busetto, L., Dicker, D., De Groot, M., Eisenberg, D., Flint, S. W., … Dixon, J. B. (2020). Joint international consensus statement for ending stigma of obesity. Nature Medicine, 26(4), 485–497. https://doi.org/10.1038/s41591-020-0803-x
- 15Hall, K. D., Ayuketah, A., Brychta, R., Cai, H., Cassimatis, T., Chen, K. Y., Chung, S. T., Costa, E., Courville, A., Darcey, V., Fletcher, L. A., Forde, C. G., Gharib, A. M., Guo, J., Howard, R., Joseph, P. V., McGehee, S., Ouwerkerk, R., Raisinger, K., … Zhou, M. (2019). Ultra-Processed Diets Cause Excess Calorie Intake and Weight Gain: An Inpatient Randomized Controlled Trial of Ad Libitum Food Intake. Cell Metabolism, 30(1), 67-77.e3. https://doi.org/10.1016/j.cmet.2019.05.00
- 16Javed, Z., Valero-Elizondo, J., Maqsood, M. H., Mahajan, S., Taha, M. B., Patel, K. V., Sharma, G., Hagan, K., Blaha, M. J., Blankstein, R., Mossialos, E., Virani, S. S., Cainzos-Achirica, M., & Nasir, K. (2022). Social determinants of health and obesity: Findings from a national study of US adults. Obesity, 30(2), 491–502. https://doi.org/10.1002/oby.23336
- 17Pan, L., Sherry, B., Njai, R., & Blanck, H. M. (2012). Food Insecurity Is Associated with Obesity among US Adults in 12 States. Journal of the Academy of Nutrition and Dietetics, 112(9), 1403–1409. https://doi.org/10.1016/j.jand.2012.06.011
- 18Browne, N. T., Hodges, E. A., Small, L., Snethen, J. A., Frenn, M., Irving, S. Y., Gance-Cleveland, B., & Greenberg, C. S. (2022). Childhood obesity within the lens of racism. Pediatric Obesity, 17(5), e12878. https://doi.org/10.1111/ijpo.12878
- 19Kumanyika, S. K. (2022). Advancing Health Equity Efforts to Reduce Obesity: Changing the Course. Annual Review of Nutrition, 42(1). https://doi.org/10.1146/annurev-nutr-092021-050805
- 20Golden, N. H., Schneider, M., Wood, C., Committee on Nutrition, Committee on Adolescence, & Section on Obesity. (2016). Preventing Obesity and Eating Disorders in Adolescents. Pediatrics, 138(3), e20161649. https://doi.org/10.1542/peds.2016-1649
- 21Laraia, B. A., Leung, C. W., Tomiyama, A. J., Ritchie, L. D., Crawford, P. B., & Epel, E. S. (2021). Drive for thinness in adolescents predicts greater adult BMI in the Growth and Health Study cohort over 20 years. Obesity (Silver Spring, Md.), 29(12), 2126–2133. https://doi.org/10.1002/oby.23285
- 22Jacquet, P., Schutz, Y., Montani, J.-P., & Dulloo, A. (2020). How dieting might make some fatter: Modeling weight cycling toward obesity from a perspective of body composition autoregulation. International Journal of Obesity, 44(6), 1243–1253. https://doi.org/10.1038/s41366-020-0547-1
- 23Pietiläinen, K. H., Saarni, S. E., Kaprio, J., & Rissanen, A. (2012). Does dieting make you fat? A twin study. International Journal of Obesity, 36(3), 456–464. https://doi.org/10.1038/ijo.2011.160
- 24Tomiyama, A. J., Carr, D., Granberg, E. M., Major, B., Robinson, E., Sutin, A. R., & Brewis, A. (2018). How and why weight stigma drives the obesity “epidemic” and harms health. BMC Medicine, 16(1), 123. https://doi.org/10.1186/s12916-018-1116-5
- 25Chu, W. W.-E., & Chu, N.-F. (2021). Adverse childhood experiences and development of obesity and diabetes in adulthood-A mini review. Obesity Research & Clinical Practice, 15(2), 101–105. https://doi.org/10.1016/j.orcp.2020.12.010
Image Credits
- Fig 7.17. “Obesity Trends Among U.S. Adults, BRFSS, 1990-2010” by Division of Nutrition, Physical Activity, and Obesity, National Center for Chronic Disease Prevention and Health Promotion, Centers for Disease Control and Prevention is in the Public Domain
- Fig 7.18. https://www.cdc.gov/obesity/data/maps/2020/overall-2011-2020-508.pptx by Division of Nutrition, Physical Activity, and Obesity, National Center for Chronic Disease Prevention and Health Promotion, Centers for Disease Control and Prevention is in the Public Domain
- Fig 7.19. “Trends in obesity prevalence” by National Center for Health Statistics is in the Public Domain
- Fig 7.20. Elements of obesogenic environment: “wocintech” by WOCinTech Chat is licensed under CC BY 2.0; “Perfect timing” by Tamara Menzi, Unsplash is in the Public Domain, CC0; “Vending machines” by Purchase College Library is licensed under CC BY-NC 2.0
Economic and social circumstances, such as poverty and racism, that impact health.
Areas where healthy foods simply aren’t available or easily accessible.
Having consistent access to enough food for an active, healthy life.
Having inconsistent access to enough food for an active, healthy life.
Beliefs continuously promoted by diet companies, media, and influencers that center the idea that being thin is the same as being healthy, and that anyone who applies themselves by eating the right foods in the right amounts can achieve that ideal.

{kind=link}