Fats serve useful functions in both the body and the diet. In the body, fat functions as an important depot for energy storage, offers insulation and protection, and plays important roles in regulating and signaling. Large amounts of dietary fat are not required to meet these functions, because most fat molecules can be synthesized by the body from other organic molecules like carbohydrate and protein (with the exception of two essential fatty acids). However, fat also plays unique roles in the diet, including increasing the absorption of fat-soluble vitamins and contributing to the flavor and satisfaction of food. Let’s take a closer look at each of these functions of fats in the body and in the diet.
The Functions of Fats in the Body
Storing Energy
The excess energy from the food we eat is incorporated into adipose tissue, or fatty tissue. Most of the energy required by the human body is provided by carbohydrates and lipids. As discussed in the Carbohydrates unit, glucose is stored in the body as glycogen. While glycogen provides a ready source of energy, it is quite bulky with heavy water content, so the body cannot store much of it for long. Fats, on the other hand, can serve as a larger and more long-term energy reserve. Fats pack together tightly without water and store far greater amounts of energy in a reduced space. A fat gram is densely concentrated with energy, containing more than double the amount of energy as a gram of carbohydrate.
We draw on the energy stored in fat to help meet our basic energy needs when we’re at rest and to fuel our muscles for movement throughout the day, from walking to class, playing with our kids, dancing through dinner prep, or powering through a shift at work. Historically, when humans relied on hunting and gathering wild foods or on the success of agricultural crops, having the ability to store energy as fat was vital to survival through lean times. Hunger remains a problem for people around the world, and being able to store energy when times are good can help them endure a period of food insecurity. In other cases, the energy stored in adipose tissue might allow a person to weather a long illness.
Unlike other body cells that can store fat in limited supplies, fat cells are specialized for fat storage and are able to expand almost indefinitely in size. An overabundance of adipose tissue can be detrimental to your health not only from mechanical stress on the body due to excess weight, but also from hormonal and metabolic changes. Obesity can increase the risk for many diseases, including type 2 diabetes, heart disease, stroke, kidney disease, and certain types of cancer. It can also interfere with reproduction, cognitive function, and mood. Thus, while some body fat is critical to our survival and good health, in large quantities it can be a deterrent to maintaining good health.
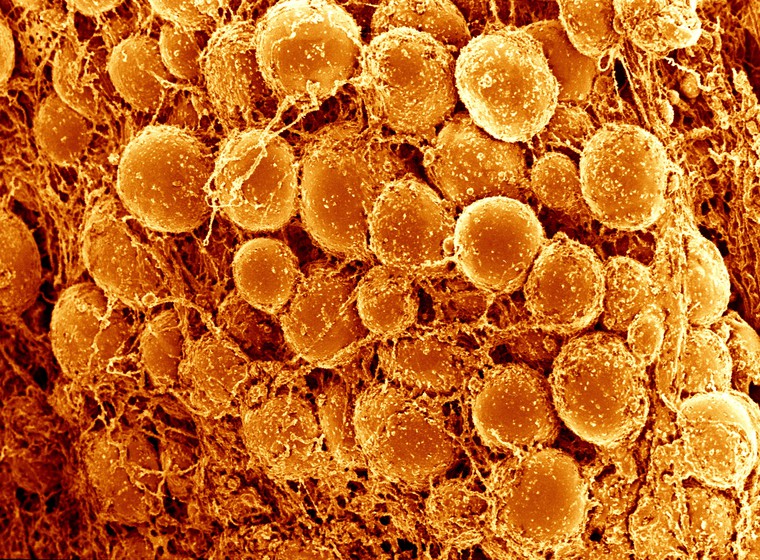
Figure 5.3. Scanning electron micrograph of adipose tissue, showing adipocytes. Computer-coloured orange.
Insulating and Protecting
The average body fat for a man is 18 to 24 percent and for a woman is 25 to 31 percent1, but adipose tissue can comprise a much larger percentage of body weight depending on the degree of obesity of the individual. Some of this fat is stored within the abdominal cavity, called visceral fat, and some is stored just underneath the skin, called subcutaneous fat. Visceral fat protects vital organs—such as the heart, kidneys, and liver. The blanket layer of subcutaneous fat insulates the body from extreme temperatures and helps keep the internal climate under control. It pads our hands and buttocks and prevents friction, as these areas frequently come in contact with hard surfaces. It also gives the body the extra padding required when engaging in physically demanding activities such as ice skating, horseback riding, or snowboarding.
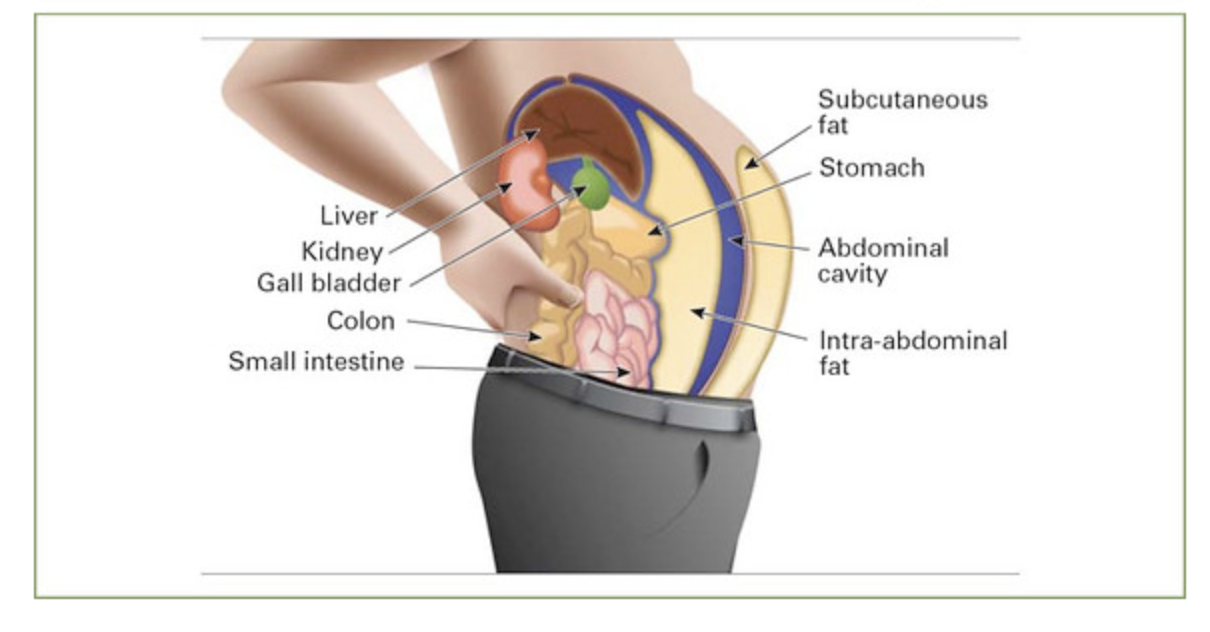
Figure 5.4. There are two types of fat stored as adipose tissue: subcutaneous fat and visceral fat.
Regulating and Signaling
Fats help the body to produce and regulate hormones. For example, adipose tissue secretes the hormone leptin, which signals the body’s energy status and helps to regulate appetite. Fat is also required for reproductive health; a woman who lacks adequate amounts may stop menstruating and be unable to conceive until her body can store more energy as fat. Omega-3 and omega-6 essential fatty acids help regulate cholesterol and blood clotting and control inflammation in the joints, tissues, and bloodstream. Fats also play important functional roles in sustaining nerve impulse transmission, memory storage, and tissue structure. Lipids are especially focal to brain activity in structure and in function, helping to form nerve cell membranes, insulate neurons, and facilitate the signaling of electrical impulses throughout the brain.
The Function of Fats in THE DIET
Aiding Absorption and Increasing Bioavailability
The dietary fats in the foods we eat aid in the transport of fat-soluble vitamins, carrying them through the digestive process and improving their intestinal absorption. This improved absorption is known as increased bioavailability. Dietary fats can also increase the bioavailability of compounds known as phytochemicals—non-essential plant compounds considered beneficial to human health. Many phytochemicals are fat-soluble, such as lycopene found in tomatoes and beta-carotene found in carrots, so dietary fat improves the absorption of these molecules in the digestive tract.
In addition to improving bioavailability of fat-soluble vitamins, some of the best dietary sources of these vitamins are also foods that are high in fat. For example, good sources of vitamin E are nuts (including peanut butter and other nut butters), seeds, and plant oils such as those found in salad dressings, and it’s difficult to consume enough vitamin E if you’re eating a very low-fat diet. (Although fried foods are usually cooked in vegetable oils, vitamin E is destroyed by high heat, so you won’t find a lot of vitamin E in french fries or onion rings. Your best bets are minimally-processed, whole foods.) Vegetable oils also provide some vitamin K, and fatty fish and eggs are good sources of vitamins A and D.
Contributing to the Smell, Taste, and Satiety of Foods
Fats satisfy appetite (the desire to eat) because they add flavor to foods. Fat contains dissolved compounds that contribute to mouth-watering aromas and flavors. Fat also adds texture, making baked foods moist and flakey, fried foods crispy, and adding creaminess to foods like ice cream and cream cheese. Consider fat-free cream cheese; when fat is removed from the cream, much of the flavor is also lost. As a result, it is grainy and flavorless—nothing like its full-fat counterpart—and many additives are used in an attempt to replace the lost flavor.

Fats satisfy hunger (the need to eat) because they’re slower to be digested and absorbed than other macronutrients. Dietary fat thus contributes to satiety—the feeling of being satisfied or full. When fatty foods are swallowed, the body responds by enabling the processes controlling digestion to slow the movement of food along the digestive tract, giving fats more time to be digested and absorbed and promoting an overall sense of fullness. Sometimes, before the feeling of fullness arrives, people overindulge in fat-rich foods, finding the delectable taste irresistible. Slowing down to appreciate the taste and texture of foods can give your body time to send signals of satiety to your brain, so you can eat enough to be satisfied without feeling overly full.

Providing Essential Fatty Acids
Most lipid molecules can be synthesized in the body from other organic molecules, so they don’t specifically need to be provided in the diet. However, there are two that are considered essential and must be included in the diet: linoleic acid and alpha-linolenic acid. We’ll discuss these two fatty acids in detail later in the unit.
Self-Check:
Attributions:
- University of Hawai‘i at Mānoa Food Science and Human Nutrition Program, “The Function of Lipids in the Body,” CC BY-NC 4.0
References:
- ACE (2009) What are the guidelines for percentage of body fat loss? American Council on Exercise (ACE). Ask the Expert Blog. December 2, 2009.
- Obesity Prevention Source. Harvard T.H. Chan School of Public Health. Health Risks: Weight Problems Take a Hefty Toll on Body and Mind. Retrieved from: https://www.hsph.harvard.edu/obesity-prevention-source/obesity-consequences/health-effects/
Images:
- Figure 5.3. “Adipose tissue, close-up showing adipocytes, SEM” by David Gregory & Debbie Marshall is licensed under CC BY 4.0
- Figure 5.4. “Pandemic of Lifestyle Disease” by Sandra Cohen-Rose and Colin Rose is licensed under CC-BY-2.0
- “French Fries in Paris” by Jim Larrison is licensed under CC BY 2.0
- “Eating a Burger Jonny B’z Dog and More Lourdie Dinner March 24, 20116” by Steven Depolo is licensed under CC-BY-2.0
Not so long ago, food choices were limited to what could be grown or raised, hunted or gathered. Today, grocery stores offer seemingly infinite choices in foods, with entire aisles dedicated to breakfast cereals and cases filled with a multitude of different yogurts. Faced with so many choices, how can we decide? Taste matters, of course. But if a healthy diet is your goal, so does nutrition. Food labels are our window into the nutritional value of a given food. Let’s examine what we can learn from food labels and how reading them can help us make smart choices to contribute to a healthy diet.

The U.S. Food and Drug Administration (FDA) requires food manufacturers to accurately label foods so that consumers can be informed about their contents. There are 5 types of information required by the FDA on every food label, except for fresh produce and seafood1.2:
- Statement of identity (what type of food is it?)
- Net contents of the package (how much is in there?)
- Name and address of manufacturer (where was it produced?)
- Ingredients list (what ingredients are included in the food?)
- Nutrition information (what is the amount of nutrients included in a serving of food?)
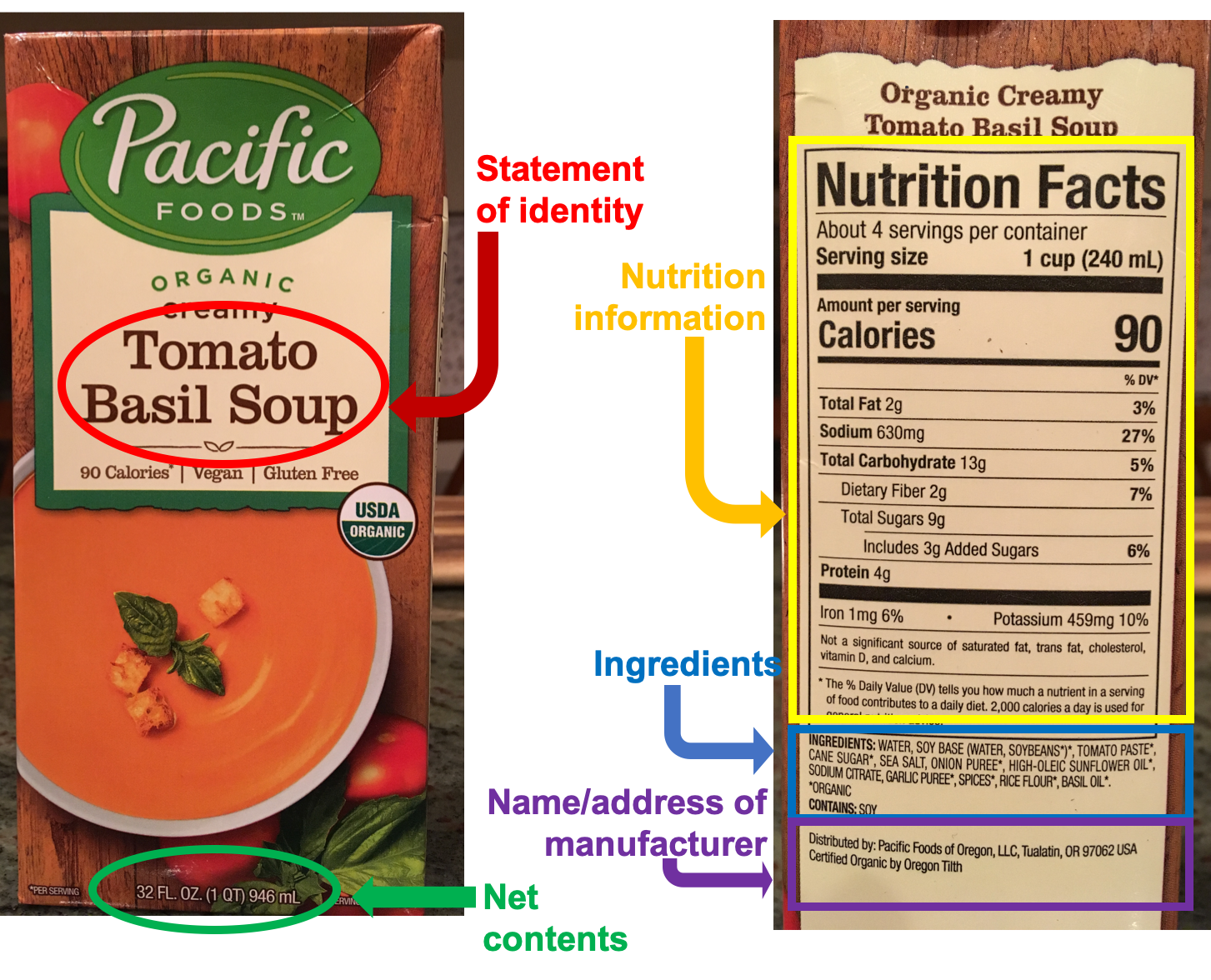
Figure 1.12. The 5 required types of information on a food label.
The statement of identity and net contents of the package tell you what type of food you’re purchasing and how much is in the package. The name and address of the manufacturer are important if there’s a food recall due to an outbreak of foodborne illness or other contamination issue. Given the size of our food system and the fact that one manufacturer may make products packaged under multiple brand names, being able to trace a food’s origin is critical.
The last two types of required information—the ingredients list and the nutrition information—are a bit more complex and provide valuable information to consumers, so let’s look more closely at each of these parts of a food label.
Ingredients List
![A photo of the ingredients listed on a cornbread mix. It reads "INGREDIENTS: Enriched unbleached flour (wheat flour, malted barley flour, ascorbic acid [dough conditioner], niacin, reduced iron, thiamin mononitrate, riboflavin, folic acid), sugar, degermed yellow cornmeal, salt, leavening (baking soda, sodium acid pyrophosphate), soybean oil, honey powder, natural flavor. CONTAINS: Wheat. May contain milk, eggs, soy and tree nuts.](https://openwa.pressbooks.pub/app/uploads/sites/295/2023/03/image3-3.png) The ingredients list includes all ingredients, listed from most predominant to least predominant (by weight) in the product. For example, in the corn muffin mix label to the right, the most prevalent ingredient is enriched unbleached flour (with ingredients in the flour then listed in parentheses), followed by sugar, cornmeal, salt, and then a few other ingredients.
The ingredients list includes all ingredients, listed from most predominant to least predominant (by weight) in the product. For example, in the corn muffin mix label to the right, the most prevalent ingredient is enriched unbleached flour (with ingredients in the flour then listed in parentheses), followed by sugar, cornmeal, salt, and then a few other ingredients.
This order of ingredients comes in handy when judging the nutritional value of a product. For example, in the ingredients list for the corn muffin mix shown at right, it’s interesting to note that it contains more sugar than cornmeal! The ingredients list can also help you determine whether a bread contains more whole grain flour than refined flour. Or, if you’re choosing a breakfast cereal and the first ingredient is sugar, that’s a red flag that it’s more of a dessert than part of a nutritious breakfast.
By law, food manufacturers must also list major allergens, which include milk, egg, fish, crustacean shellfish, tree nuts, wheat, peanuts, and soybeans.2 Allergens may be listed in a separate statement, as on the corn muffin mix label, which lists “Contains: Wheat” on the label. Alternatively, allergens can be listed in parentheses within the ingredient list, such as “lecithin (soy).” Some labels include an optional “may contain” or “made in shared equipment with…” statement that lists additional allergens that could be present, not as ingredients in the food, but in trace amounts from equipment contamination. For people with food allergies, having this information clearly and accurately displayed on food packages is vital for their safety.
The Nutrition Facts Panel
If you want to learn about the nutritional value of a food, the Nutrition Facts panel is where you’ll find this information. It’s very useful for comparing products and for identifying foods that will be more or less valuable in meeting your nutritional goals. For example, if you’re trying to watch your intake of added sugar or saturated fat, or you’re trying to incorporate more dietary sources of calcium and vitamin D, the Nutrition Facts panel is a valuable tool. There are 4 main parts of a Nutrition Facts panel, shown in the figure below. The colors are added to highlight different sections of a label; Nutrition Facts are printed in black and white.
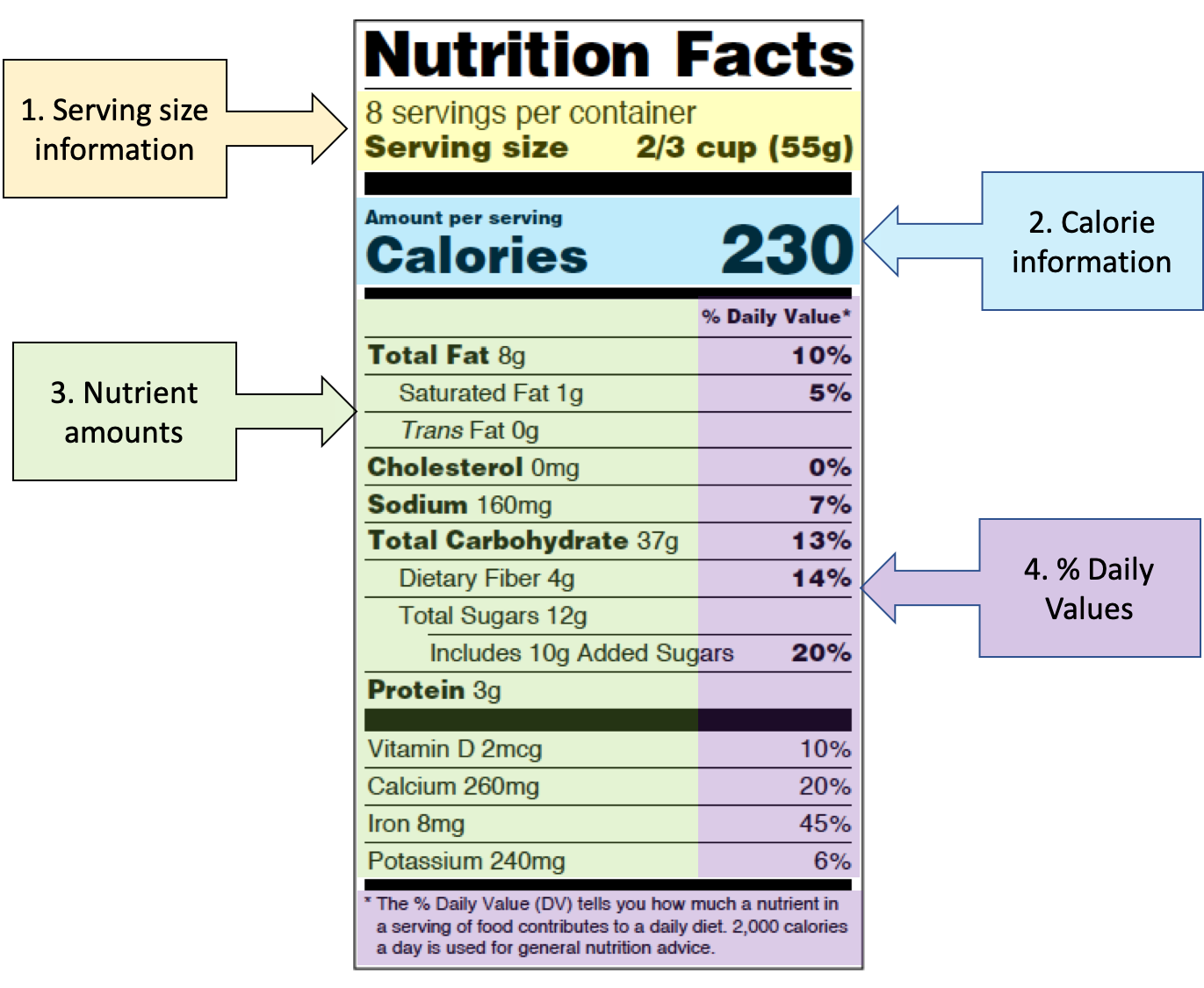
Figure 1.13. The four main sections of a Nutrition Facts label, highlighted in color.
1. Serving size information
It’s fitting that serving size information is first on the Nutrition Facts panel, because all of the information that follows is based on it. The serving size of the food is the amount that is customarily eaten at one time, and all of the nutrition information on the label is based on one serving of the food. This section of the label also states the number of servings per container.1
It’s important to note that you might not always eat one serving of a food; sometimes you might eat half of a serving, and sometimes you might eat two or more servings in one sitting. For example, if the label above is for a breakfast cereal, you might easily consume 1 ⅓ cups of cereal for breakfast. If you’re interested in how many calories or nutrients you’re consuming, you would need to double the nutrition values to accurately represent your breakfast, since the serving size is only ⅔ cup.
2. Calorie information
This section simply states the number of calories, or the amount of energy, provided in one serving of the food. Again, if you consume more or less than the serving size, you’ll need to take that into consideration when estimating the calories you’re consuming.
3. Nutrient amounts
The Nutrition Facts panel must list the amounts of these nutrients: total fat, saturated fat, trans fat, cholesterol, sodium, total carbohydrate, dietary fiber, sugars, added sugars, protein, calcium, vitamin D, iron, and potassium.1
Manufacturers may also choose to add several other optional nutrients or nutritional information: calories from saturated fat, polyunsaturated fat, monounsaturated fat, soluble and insoluble fiber, sugar alcohol, other carbohydrate, and other vitamins and minerals.
4. Percent Daily Values
The Daily Value (DV) is an approximate recommendation for daily intake for a nutrient, developed by the FDA for use on food labels so that consumers can see how much of a nutrient is provided by a serving of a food relative to about how much they need each day. The DV is similar to the RDA or AI, except that because it’s used on food labels, it needs to be a simplified recommendation, with just one value rather than several for different age groups and sex, as found in the DRI.3
Most DVs are based on amounts for people age 4 years through adult, though there are DVs established for infants, toddlers, and pregnant and lactating women, and you’ll see those used on food products specifically developed for those groups. Most of the time, the DV for a nutrient is the highest RDA or AI for the group it’s intended for.
The value printed on the Nutrition Facts panel is the percent DV, which tells you how much one serving of the food contributes towards meeting the daily requirement for that nutrient.
The FDA uses the following definitions for interpreting the %DV on food labels:4
- 5%DV or less means the food is low in a nutrient.
- 10% to 19%DV means the food is a “good source” of a nutrient.
- 20%DV or greater means the food is high in a nutrient.
The DV is not as precise as the RDA, so while the %DV is useful for comparing food products or making quick judgements about the nutritional value of a food, it’s better to use the RDA if you’re looking for your individual nutrient requirements.
Putting the Nutrition Facts panel to work for you
How you use the Nutrition Facts on food labels depends on your dietary goals. If you’re trying to reduce your saturated fat intake, you’ll want to pay close attention to the %DV for saturated fat and try to choose foods with less than 5% DV for saturated fat. If you’re watching your caloric intake, you’ll want to pay attention to the calorie information. Regardless, always start by checking the serving size and comparing it to the amount you usually consume.
As an example of smart label reading, take a look at the two soup labels below. First, think about how much soup you would usually consume. There are two servings per can, but would you eat the entire can or just half of it? Many people would eat the whole can, and if that’s you, you would want to double all of the calorie and nutrient information. Both soups provide 160 calories per one-cup serving, or 320 calories for the entire can.
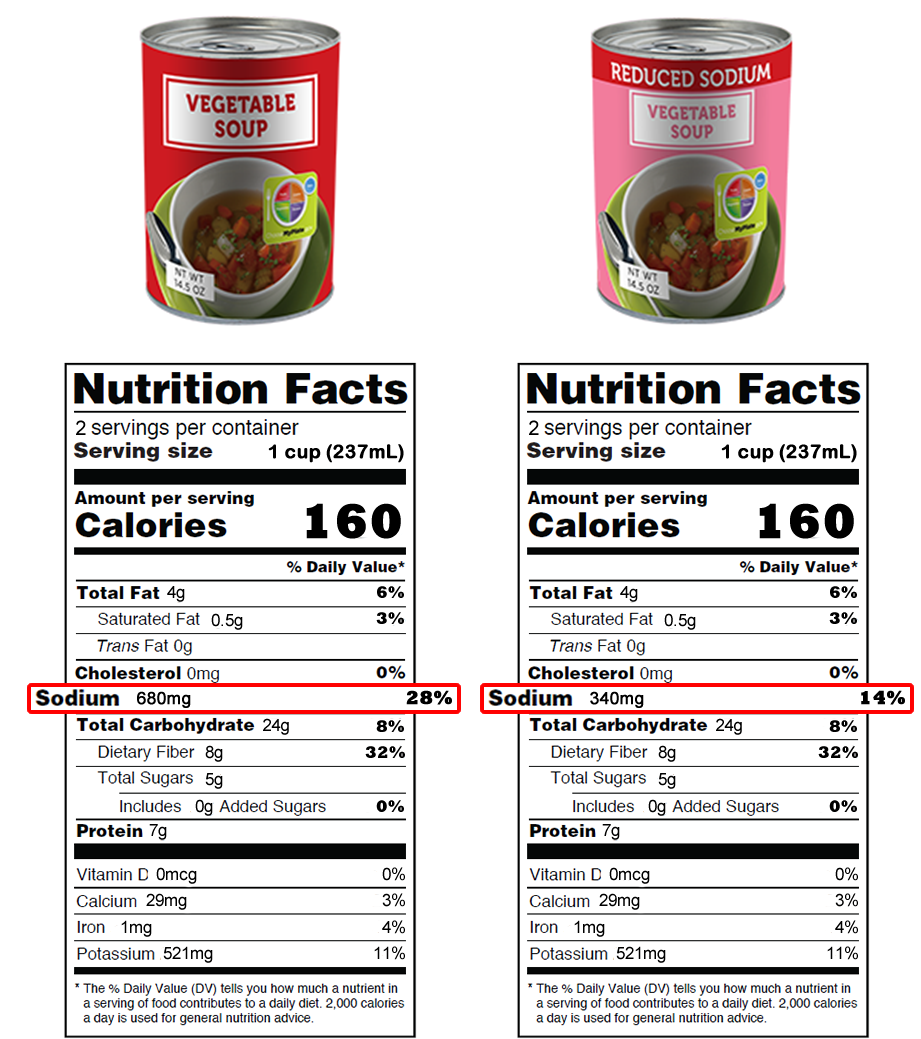
Figure 1.14. Comparison of Nutrition Facts for a regular vegetable soup, and reduced sodium vegetable soup.
Next, take a look at the sodium. Most Americans consume too much sodium, and this can increase the risk of developing high blood pressure. The regular soup has 680 mg or 28% of the DV for sodium. If you eat the entire can, that becomes 1360 mg or 56% DV. That’s a lot of sodium. You can see how the reduced sodium soup might be the wiser choice here.
VIDEO: “Reading Food Labels,” by Cincinnati Children’s, YouTube (May 9, 2019), 2:56 minutes.
What’s That Claim?
In addition to the FDA-required information on food labels, it’s common for them to be peppered with claims about the nutrient content of the food and the purported health benefits of eating it. These claims are marketing tools for food manufacturers, and they’re regulated by the FDA in an effort to ensure that they give the consumer accurate, science-based information about the food. Let’s look at the different types of claims that you’ll find on food packages.
Nutrient Claims
Nutrient claims provide straight-forward information about the level of a nutrient or calories in the food, such as “fat-free,” “low calorie,” or “reduced sodium.” Nutrient claims are regulated by the FDA, with very specific requirements for each one. For example, a food with a “low sodium” claim must have 140 mg of sodium or less per serving, whereas a food with a “reduced sodium” claim must have at least 25 percent less sodium than the standard product. You’ll see claims that a food is “high in,” “rich in,” and “excellent source of” a nutrient, all of which mean that a serving of the food contains 20% DV or more. A “good source of” claim contains 10-19% DV of the nutrient.1
 Figure 1.15. Examples of food packaging with nutrient claims. Can you spot them?
Figure 1.15. Examples of food packaging with nutrient claims. Can you spot them?
Health Claims
Health claims are statements on food packaging that link the food or a component in the food to reducing the risk of a disease. Health claims can be “authorized” or “qualified.” Authorized health claims have stronger scientific evidence to back them than qualified health claims.5
As an example of an authorized health claim, a food that is low in sodium (per the FDA’s definition of less than 140 mg per serving) can include the following claim on their packaging: “Diets low in sodium may reduce the risk of high blood pressure, a disease associated with many factors.”1
For an authorized health claim to be approved by the FDA, the agency says “there must be significant scientific agreement (SSA) among qualified experts that the claim is supported by the totality of publicly available scientific evidence for a substance/disease relationship. The SSA standard is intended to be a strong standard that provides a high level of confidence in the validity of the substance/disease relationship.”5 In other words, the FDA requires a great deal of evidence before allowing food manufacturers to claim that their products can reduce the risk of a disease. As is evident in the low sodium claim, they also require careful language, such as “may reduce” (not definitely!) and “a disease associated with many factors” (as in, there are many other factors besides sodium that influence blood pressure, so a low sodium diet isn’t a guaranteed way to prevent high blood pressure).
Qualified health claims have some evidence to support them, but not as much, so there’s less certainty that these claims are true. The FDA reviews the evidence for a qualified claim and determines how it should be worded to convey the level of scientific certainty for it. Here’s an example of a qualified health claim: “Scientific evidence suggests but does not prove that eating 1.5 ounces per day of most nuts [such as name of specific nut] as part of a diet low in saturated fat and cholesterol may reduce the risk of heart disease.”
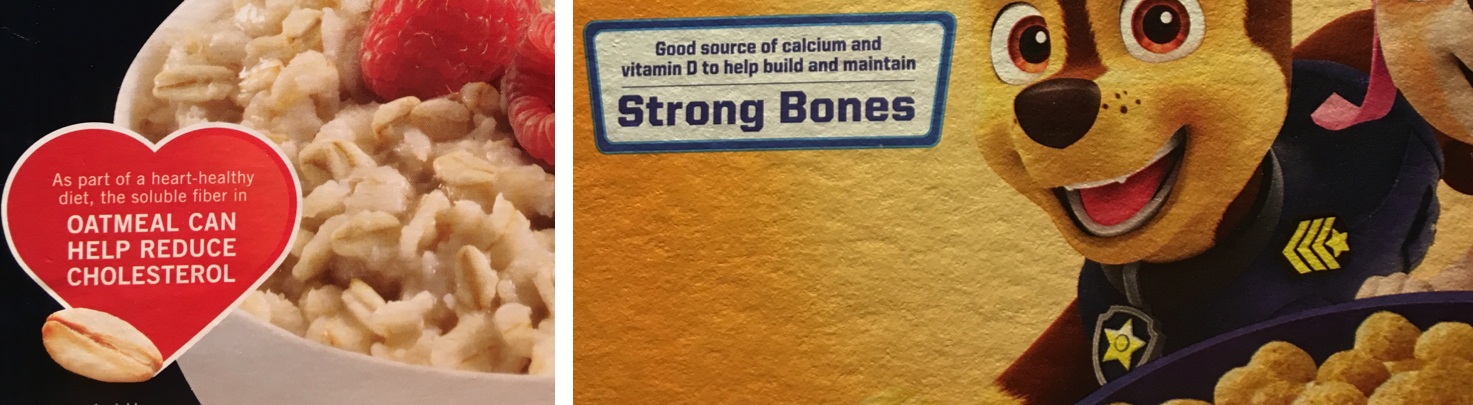
Figure 1.16. Examples of food packaging with authorized health claims. Can you spot them?
Structure-Function Claims
Health claims are very specific and precise in their language, and they convey the level of scientific certainty supporting them. In contrast, structure-function claims are intentionally vague statements about nutrients playing some role in health processes. Examples of structure-function claims are “calcium builds strong bones” and “fiber maintains bowel regularity.” Note that these statements make no claims to prevent osteoporosis or treat constipation, because structure-function claims are not allowed to say that a food or nutrient will treat, cure, or prevent any disease.6 They’re allowed by the FDA, but not specifically approved or regulated, as long as their language stays within those rules.

Figure 1.17. Examples of food and supplement packaging with structure-function claims. Can you spot them?
Structure-function claims were originally designed to be used on dietary supplements, but they can also be used on foods, and they’re usually found on foods that are fortified with specific nutrients. They are marketing language, and because nutrients are involved in so many processes, they really don’t mean much.
As you look at food labels, pay attention to what’s shown on the front of the package compared with the back and side of the package. Nutrient and health claims are usually placed strategically on the front of the package, in large, colorful displays with other marketing messages, designed to sell you the product. But for consumers trying to decide which product to buy, you’ll find the most useful information by turning the package around to read the Nutrition Facts panel and ingredients list. These parts of the label may appear more mundane, but if you understand how to read them, you’ll find that they’re rich in information.
Self-Check:
References:
- 1U.S. Food and Drug Administration. (2013, January). A Food Labeling Guide: Guidance for Industry. Retrieved January 2, 2020, from FDA website: https://www.fda.gov/regulatory-information/search-fda-guidance-documents/guidance-industry-food-labeling-guide
- 2U.S. Food and Drug Administration. (2019, December 11). Food Labeling & Nutrition. Retrieved December 18, 2019, from FDA website: http://www.fda.gov/food/food-labeling-nutrition
- 3National Institutes of Health, Office of Dietary Supplements. (n.d.). Daily Values (DVs). Retrieved December 22, 2019, from https://ods.od.nih.gov/HealthInformation/dailyvalues.aspx
- 4U.S. Food and Drug Administration. (2019, September 5). New and Improved Nutrition Facts Label. Retrieved January 2, 2020, from FDA website: http://www.fda.gov/food/nutrition-education-resources-materials/new-and-improved-nutrition-facts-label
- 5U.S. Food and Drug Administration. (2018). Questions and Answers on Health Claims in Food Labeling. FDA. Retrieved from http://www.fda.gov/food/food-labeling-nutrition/questions-and-answers-health-claims-food-labeling
- 6U.S. Food and Drug Administration. (2018). Structure/Function Claims. FDA. Retrieved from http://www.fda.gov/food/food-labeling-nutrition/structurefunction-claims
Image Credits:
- Grocery aisle photo by NeONBRAND on Unsplash (license information)
- Figure 1.12. “The 5 required types of information on a food label” by Alice Callahan is licensed under CC BY-NC 4.0
- “Corn muffin ingredient list” by Alice Callahan is licensed under CC BY-NC 4.0
- Figure 1.13. Part of a nutrition fact label by Alice Callahan, CC BY 4.0, edited from "Nutrition Facts Label" by C.D.C. is in the Public Domain
- Figure 1.14. "Soup label comparison" by U.S.D.A. ChooseMyPlate is in the Public Domain
- Figure 1.15. "Examples of food packaging with nutrient claims" by Alice Callahan is licensed under CC BY-NC 4.0
- Figure 1.16. "Examples of food packaging with authorized health claims" by Alice Callahan is licensed under CC BY-NC 4.0
- Figure 1.17. "Examples of food packaging with structure-function claims" by Alice Callahan is licensed under CC BY-NC 4.0
By this point in the unit, you should understand the types of studies used in nutrition research and the quality of evidence each can provide. As you sift through studies, there are a few limitations of nutrition research that are always worth keeping in mind:
- Challenges in nutrition research: There are some inherent challenges to researching what people eat and how it affects their health. This fact limits the quality of evidence and stirs controversy in nutrition research.
- Influence of food industry funding: Because government funding for nutrition research is limited, much of it is funded by the food industry. Industry’s primary goal is to sell more of their products, so they have a conflict of interest that can result in bias in the way they design studies and interpret the results.
Being alert to these two things means always examining nutrition research with a healthy sense of skepticism. Let’s take a closer look at these two issues in nutrition science.

Challenges in Nutrition Research
How does the food we eat affect our health? This question is exceedingly difficult to answer with certainty. We all need to eat every day, but we can choose from a huge array of possible foods in different combinations. And it’s probably not what we eat on any given day that matters, but what we eat over months and years and decades—our long-term eating patterns—that matter to our long-term health.
Imagine that you’re a nutrition researcher, and you’ve made the observation that over the last 50 years in the U.S., people have been consuming more and more processed foods (foods made with refined ingredients and industrial processes, usually with the addition of sugar, fat, and/or salt). You hypothesize that processed foods are contributing to obesity, which has also increased over the last 50 years. You might first test your hypothesis in animal studies by feeding mice and rats a buffet of potato chips, soda, and Twinkies, and measuring changes in their body weight. You might find that the animals do, in fact, gain weight on this diet. However, you know that what is true in rodents isn’t always true in humans, and you’ll need to study humans in order to understand the role of processed foods in the obesity epidemic.
Your next step might be to conduct an observational study, the most common type of study design in human nutrition research. For example, you might do a cross-sectional study where you compare groups of people who eat a lot of processed foods with those who eat very little. Or you might conduct a prospective cohort study in which you ask people how much processed foods they eat and then follow them over time, looking for correlations between processed food consumption and their body composition.
These types of studies have been conducted, and they’ve found correlations between consumption of processed foods and obesity. For example, a cross-sectional study published in 2018 compared the consumption of processed foods and the prevalence of obesity in 19 European countries and found that countries where people eat more processed foods also have a greater prevalence of obesity.1 A prospective cohort study published in 2016 followed nearly 8,500 university graduates in Spain and found that those who ate more processed foods were more likely to be overweight or obese 9 years later.2
From these results, can we conclude that eating more processed food causes weight gain? Nope. It’s a tempting conclusion, but this brings us to the first major problem with nutrition research: Observational studies can only show that two variables (eating processed foods and obesity, in this case) are correlated, not that one causes the other. This distinction is especially important in nutrition because diet is intertwined with many other lifestyle and socioeconomic factors that also affect health outcomes. For example, people who eat more processed food might also eat fewer fruits and vegetables, exercise or sleep less, have more stress, or have less access to preventative healthcare. These are just a few of the confounding factors that could explain the observed correlation between processed food consumption and weight gain. Weight gain might have nothing to do with processed food and instead be driven by one or all of these factors, or others that we haven’t considered.
The second major problem with observational nutrition research is that it’s difficult to accurately quantify what and how much people eat, especially over long periods of time. Epidemiological studies usually rely on questionnaires that ask people to remember how much food they ate, but people are notoriously bad at remembering this type of information, and sometimes we fudge the truth. For example, you might remember that you had a cup of coffee but forget that you added cream, completely forget about a mid-morning muffin snack, or guess that you ate 2 cups of veggies when it was closer to 1.5 cups. And many diet questionnaires, called food frequency questionnaires, ask people to recollect and mentally average their food and beverage intake for the last 12 months, not just yesterday. The image below shows part of a page from a 24-page National Health and Nutrition Examination Survey (NHANES) food questionnaire, a national survey often used for research on country-wide dietary patterns. As you can see, these questions are detailed, and there’s plenty of room for small errors to accumulate.
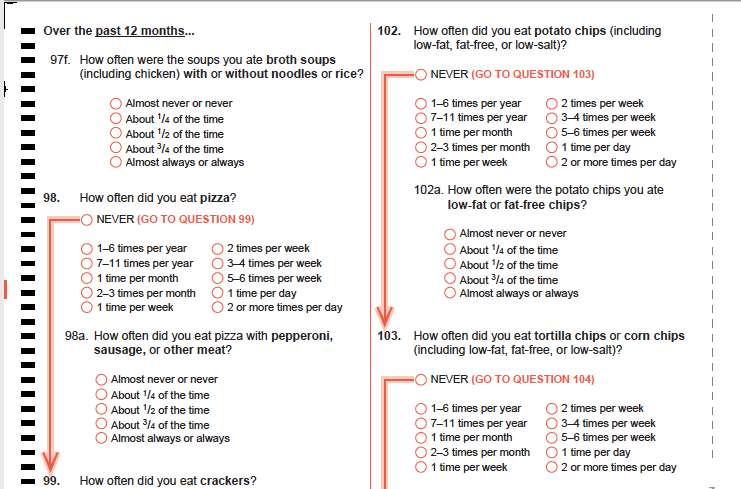
Figure 2.5. A sample page from the NHANES Food Questionnaire.
A third challenge in nutrition research is that diet is just so complex. Stanford physician and researcher John Ioannidis, a frequent critic of observational nutrition research, described the complexity of diet in a 2018 editorial published in JAMA: “Individuals consume thousands of chemicals in millions of possible daily combinations. For instance, there are more than 250,000 different foods and even more potentially edible items, with 300,000 edible plants alone.” He also points out that how an individual responds to a particular dietary pattern can be influenced by genetics, age, and the way they metabolize nutrients. “Disentangling the potential influence on health outcomes of a single dietary component from these other variable is challenging, if not impossible,” Ioannidis wrote.3

Returning to the question of processed foods, all three of these challenges impact how we interpret observational studies that show a correlation between processed food consumption and weight gain. It doesn’t mean that these studies are useless, but we want to be aware of their limitations and consider other ways to test the hypothesis. One way to overcome these challenges is to conduct a randomized controlled trial (RCT), the study design that gives us the highest quality evidence. RCTs are time and funding-intensive experiments, so they’re usually only conducted after consistent evidence from observational and laboratory studies has accumulated.
It turns out that there has been a randomized controlled trial of processed foods and weight gain. It was funded by the National Institutes of Health and published in 2019 in the journal Cell Metabolism.4 In this study, 20 participants lived in the NIH’s Clinical Center for one month, where they consumed only processed foods for two weeks and only unprocessed foods for another two weeks, and they could eat as much or as little as they liked during each of these periods. The diets were carefully designed by dietitians so that they were matched in calories, sugar, fat, fiber, and macronutrients, and the exact amounts consumed by the participants were measured every day (solving the problem of measuring diet complexity and accurately describing what and how much people eat every day).
The study found that people ate about 500 kilocalories more and gained about a pound per week when they were eating processed foods. This study design could show causation, not just correlation, because the other nutritional factors like calories, sugar, fat, fiber, and macronutrients were held constant, and the diets were tested in the same people, so other factors such as genetics, sleep, stress, and exercise were constant between the two types of diets. (This was an example of a crossover randomized controlled trial, in which each subject serves as their own control, and they completed the processed and unprocessed phases of the trial in random order.)

Figure 2.6. At left, researchers Kevin Hall and Stephanie Chung talk with one of the processed foods trial participants at the NIH Clinical Center, an inpatient facility where participants lived for the duration of the study. At right, an NIH worker prepares meals for participants in the center’s kitchen. All meals were provided for study participants to carefully control their diet during the trial.
This study suggested something very important—that food processing causes people to eat more food and gain weight. However, even the best study design has limitations. For one thing, this study was small (just 20 participants), and it only lasted for two weeks, so we don’t know if the findings apply to the general population over a lifetime of complex, ever-changing diets. The next steps will be to try to repeat the study in another group of people to see if the finding holds and to design studies to figure out why processed foods cause increased caloric intake.
As you evaluate nutrition research, especially observational studies, keep in mind the inherent challenges of nutrition research and look for randomized controlled trials that can help solve those challenges. Even for randomized controlled trials, consider their limitations, and know that one study is never enough to fully answer a question in the complex field of nutrition.
Industry Influence: Follow the Money
Understanding how diet influences health is a pressing need. By some estimates, a suboptimal diet is the single greatest changeable risk factor contributing to death and disability worldwide, and in the United States, the cost of diet-related chronic diseases are estimated to be as high as $1 trillion each year.5 Yet, for all its importance, nutrition science has long suffered from a lack of government investment, with only about 5 percent of the National Institutes of Health (NIH) budget, or $1.8 billion, directed towards research on how the foods we eat affect our health, according to a 2019 investigation by Politico. “In 2018, NIH funding for cancer, which affects just under 9 percent of the population, was $6.3 billion. Funding for obesity, which affects about 30 percent of the country, was about $1 billion,” the article noted.6
With so little government funding for nutrition science, who is funding the rest of the studies that feed the constant news cycle? Many are funded by food companies and industry groups, either to conduct studies in their own research divisions or in the form of grants given to university scientists. That’s problematic, because food companies and industry groups have an inherent bias or conflict of interest. Their primary goal is to promote their products and to sell more of them—not to advance knowledge of food and health—and this affects how they frame research questions, design and interpret studies, and report their results.
Marion Nestle, a retired nutrition professor at New York University, has written extensively about this problem. For a year in 2015-2016, she informally tracked industry-funded studies and found that 90 percent of the time, their conclusions benefitted the industry that funded them. In another example, a 2013 meta-analysis found that among studies that looked at whether soda consumption contributed to obesity, those funded by the soda industry were five times more likely to conclude that it doesn’t contribute to obesity compared to those not funded by the industry.7 (Consider the processed foods RCT we just discussed. It was funded by the National Institutes of Health, which doesn’t have a stake in the results. Would you trust the results of a study of processed foods if it was funded by Nabisco? Or for that matter, the Broccoli Growers of America? Probably not.)
There’s likely a long history of biased nutrition research influencing dietary advice. For example, in the 1960s, the sugar industry paid well-respected academic scientists to publish research concluding that it was fat—not sugar—that was detrimental to heart health.8 (Both too much fat and too much sugar can negatively affect heart health, but it benefited the sugar industry to focus the blame on fat.) As recently as 2015, Coca-Cola was funding research meant to promote lack of physical activity as the main cause of obesity, shifting blame away from dietary factors, such as drinking soda.9 When food companies drive the narrative coming out of nutrition research, this can potentially impact public policy.
Media attention has made researchers and policy makers much more aware of the problems with industry funding and conflicts of interest in nutrition research, and they’re working to solve them. But regardless, if you see reports of a study that shows that blueberries can block bladder infections, pistachios can prevent pancreatitis, or cinnamon can cure cancer… well, you should be skeptical, and always check the funding source. Studies on a single type of food are almost always industry-funded.
How to find clarity in a complex field
Let’s review some of the key issues:
- Nutrition research is really difficult to do well. We want to know how nutrition relates to health over the long term, but it’s hard to quantify how people eat over a lifetime and track them for long enough to see an impact.
- We often rely on observational studies, which can only show that two variables are correlated, not that one causes the other.
- Randomized controlled trials are rare, and they’re often small, short-term studies that may or may not tell us what happens in the real world.
- Diet is exceptionally complex, with countless combinations of different nutrients and foods.
- One study is never enough to fully answer a question in the complex field of nutrition.
- Nutrition research is often funded by the food industry, which can be biased towards results that benefit business, not human health.
All of this can be discouraging, but you should also know that researchers are working hard to improve the quality of nutrition research and to interpret it honestly for the rest of us. As a consumer of nutrition information, use a skeptical eye when you read news of the latest nutrition research. Look for areas of consensus, where committees of experts have put their heads together to come up with the best advice they can based on the evidence we have, such as in the Dietary Guidelines for Americans. You’ll find that while experts in this field are often debating the latest controversy, they also agree on a lot. As we continue on in this unit, we’ll talk more about how to find accurate sources of information and who you can trust for evidence-based advice in the field of nutrition.
Self-Check:
References
- 1Monteiro, C. A., Moubarac, J.-C., Levy, R. B., Canella, D. S., Louzada, M. L. da C., & Cannon, G. (2018). Household availability of ultra-processed foods and obesity in nineteen European countries. Public Health Nutrition, 21(1), 18–26. https://doi.org/10.1017/S1368980017001379
- 2Mendonça, R. de D., Pimenta, A. M., Gea, A., de la Fuente-Arrillaga, C., Martinez-Gonzalez, M. A., Lopes, A. C. S., & Bes-Rastrollo, M. (2016). Ultraprocessed food consumption and risk of overweight and obesity: The University of Navarra Follow-Up (SUN) cohort study. The American Journal of Clinical Nutrition, 104(5), 1433–1440. https://doi.org/10.3945/ajcn.116.135004
- 3Ioannidis, J. P. A. (2018). The Challenge of Reforming Nutritional Epidemiologic Research. JAMA, 320(10), 969–970. https://doi.org/10.1001/jama.2018.11025
- 4Hall, K. D., Ayuketah, A., Brychta, R., Cai, H., Cassimatis, T., Chen, K. Y., Chung, S. T., Costa, E., Courville, A., Darcey, V., Fletcher, L. A., Forde, C. G., Gharib, A. M., Guo, J., Howard, R., Joseph, P. V., McGehee, S., Ouwerkerk, R., Raisinger, K., … Zhou, M. (2019). Ultra-Processed Diets Cause Excess Calorie Intake and Weight Gain: An Inpatient Randomized Controlled Trial of Ad Libitum Food Intake. Cell Metabolism, 30(1), 67-77.e3. https://doi.org/10.1016/j.cmet.2019.05.008
- 5Mozaffarian, D. (2017). Conflict of Interest and the Role of the Food Industry in Nutrition Research. JAMA, 317(17), 1755–1756. https://doi.org/10.1001/jama.2017.3456
- 6Boudreau, C., & Evich, H. B. (n.d.). How Washington keeps America sick and fat. POLITICO. Retrieved January 27, 2020, from https://www.politico.com/news/agenda/2019/11/04/why-we-dont-know-what-to-eat-060299
- 7Bes-Rastrollo, M., Schulze, M. B., Ruiz-Canela, M., & Martinez-Gonzalez, M. A. (2013). Financial Conflicts of Interest and Reporting Bias Regarding the Association between Sugar-Sweetened Beverages and Weight Gain: A Systematic Review of Systematic Reviews. PLOS Medicine, 10(12), e1001578. https://doi.org/10.1371/journal.pmed.1001578
- 8Kearns, C. E., Schmidt, L. A., & Glantz, S. A. (2016). Sugar Industry and Coronary Heart Disease Research: A Historical Analysis of Internal Industry Documents. JAMA Internal Medicine, 176(11), 1680–1685. https://doi.org/10.1001/jamainternmed.2016.5394
- 9O’Connor, A. (2015, August 9). Coca-Cola Funds Scientists Who Shift Blame for Obesity Away From Bad Diets. The New York Times. https://well.blogs.nytimes.com/2015/08/09/coca-cola-funds-scientists-who-shift-blame-for-obesity-away-from-bad-diets/
Image Credits
- “Magnifying glass” photo by Emiliano Vittoriosi on Unsplash (license information)
- Figure 2.5.”NHANES food questionnaire” by CDC is in the public domain
- “Table of food photo” by Spencer Davis on Unsplash (license information)
- Figure 2.6. “NIH study center photos” by Jennifer Rymaruk, NIDDK are in the Public Domain
