The concept of energy balance seems simple: Balance the calories you consume with the calories you expend. But many factors play a role in energy intake and energy expenditure. Some of these factors are under our control and others are not. In this section, we define energy balance, look at the different components of energy expenditure, and discuss the variables that influence energy expenditure. We’ll also consider some of the factors that can affect energy intake and consider why energy balance is more complex than it seems.
Energy Balance
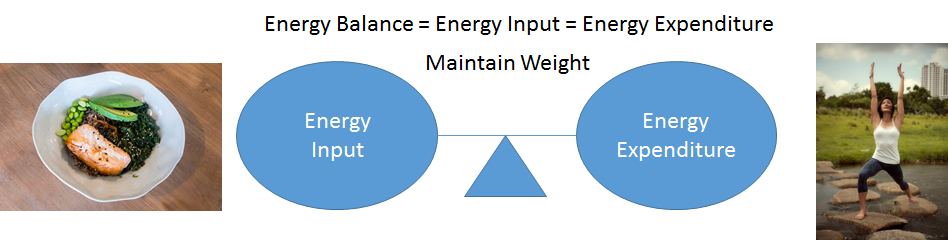
Our body weight is influenced by our energy intake (calories we consume) and our energy output (energy we expend during rest and physical activity). This relationship is defined by the energy balance equation:
Energy Balance = energy intake – energy expenditure
When an individual is in energy balance, energy intake equals energy expenditure, and weight should remain stable.
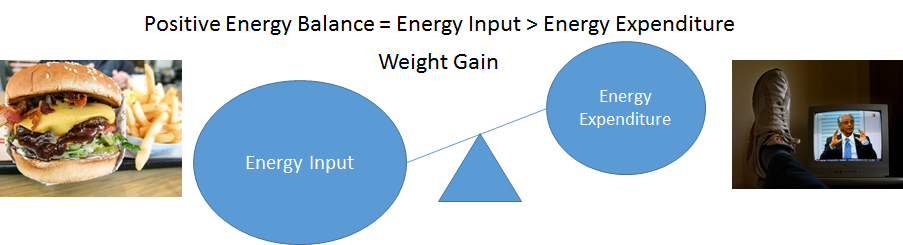
Positive energy balance occurs when energy intake is greater than energy expenditure, usually resulting in weight gain.
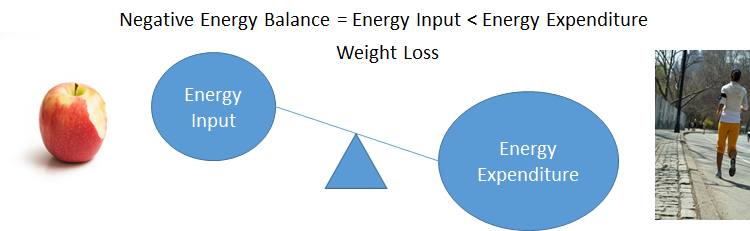
Negative energy balance is when energy intake is less than energy expenditure, usually resulting in weight loss.
Energy intake is made up of the calories we consume from food and beverages. These calories come from the macronutrients (carbohydrates, proteins, and fats) and alcohol. Remember that when the body has a surplus of energy, this energy can be stored as fat. When the body has an inadequate supply of food calories to match energy expenditure, it will turn to stored energy (i.e., adipose tissue, glycogen, and some muscle protein) to meet energy demands, resulting in weight loss.
You may see simple rules about energy balance, such as the idea that a pound of fat contains 3,500 calories, so cutting 3,500 calories from your diet will result in a pound of weight loss. This is sometimes extrapolated to say that cutting your caloric intake by 500 calories per day will lead to one pound of weight loss per week, or 52 pounds of weight loss in one year. However, this is a myth, because the body responds to caloric restriction by making adjustments to energy expenditure and resisting changes in body weight, especially over long periods of time.1
Energy balance is complex, dynamic, and variable between individuals—something we’ll explore a bit more later on this page—but it is still a vital concept in understanding body weight. Next, let’s look at the energy expenditure side of the energy balance equation, to see the components that make up energy expenditure and the factors that influence them.
Components of Energy Expenditure
The sum of caloric expenditure is referred to as total energy expenditure (TEE). There are three main components of TEE:
- Basal metabolic rate (BMR)
- Thermic effect of food (TEF)
- Physical activity
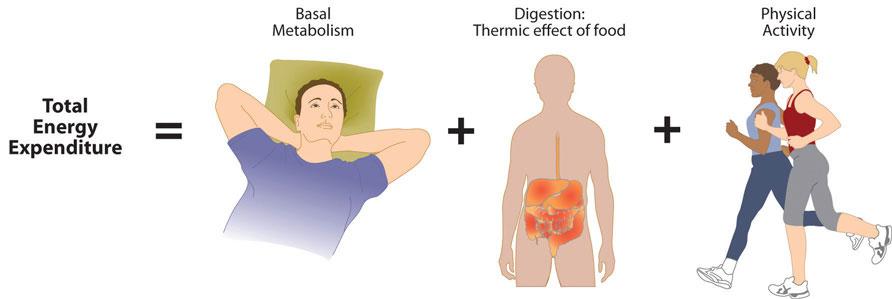
Figure 7.3. Components of total energy expenditure include basal metabolism, the thermic effect of food, and physical activity.
1. Basal Metabolic Rate (BMR)
BMR is the energy expended by the body when at rest. These are the behind-the-scenes activities that are required to sustain life. Examples include:
- respiration
- circulation
- nervous system activity
- protein synthesis
- temperature regulation
Basal metabolic rate does not include the energy required for digestion or physical activity.
BMR is usually the largest component of energy expenditure, making up about 60 to 75 percent of total energy output. For example, a sedentary person might need about 1800 calories in a day, with about 1200 of them being for BMR.
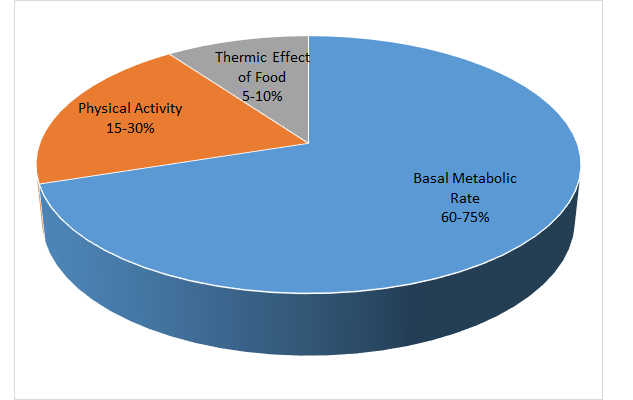
Figure 7.4. Components of energy expenditure and their percent contribution to the total in sedentary to moderately active people.
BMR can vary widely among individuals. An individual’s lean body mass—made up of organs, bone, and muscle—is the biggest determinant of BMR, because lean body tissue is more metabolically active than fat tissue. This means that a muscular person expends more energy than a person of similar weight with more fat. Likewise, increasing your muscle mass can cause an increase in your BMR. However, skeletal muscle at rest only accounts for about 18 percent of the total energy expended by lean mass. Most is used to meet the energy needs of vital organs. The liver and brain, for example, together account for nearly half of the energy expenditure by lean mass.
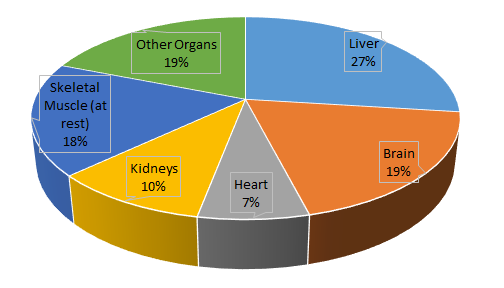
Figure 7.5. Energy expenditure of organs.
BMR depends not only on body composition but also on body size, sex, age, nutritional status, genetics, body temperature, and hormones (Table 7.1). People with a larger frame size have a higher BMR simply because they have more mass. On average, women have a lower BMR than men, because they typically have a smaller frame size and less muscle mass. As we get older, muscle mass declines, and therefore BMR declines as well.
Nutritional status also affects basal metabolism. If someone is fasting or starving, or even just cutting their caloric intake for a diet, their BMR will decrease. This is because the body attempts to maintain homeostasis and adapts by slowing down its basic functions (BMR) to help preserve energy and balance the decrease in energy intake. This is a protective mechanism during times of food shortages, but it also makes intentional weight loss more difficult.
|
Factors That Increase BMR |
Factors That Decrease BMR |
|
Higher lean body mass |
Lower lean body mass |
|
Larger frame size |
Smaller frame size |
|
Younger age |
Older age |
|
Male sex |
Female sex |
|
Stress, fever, illness |
Starvation or fasting |
|
Elevated levels of thyroid hormone |
Lower levels of thyroid hormone |
|
Pregnancy or lactation |
|
|
Stimulants such as caffeine and tobacco |
|
Table 7.1. Factors that impact BMR.
2. Thermic Effect of Food (TEF)
This is the energy needed to digest, absorb, and metabolize the nutrients in foods. It accounts for 5 to 10 percent of total energy expenditure and does not vary greatly amongst individuals.
3. Physical activity
Physical activity is another important way the body expends energy. Physical activity usually contributes anywhere from 15 to 30 percent of energy expenditure and can be further divided into two parts:
- exercise-related activity thermogenesis (EAT)
- non-exercise activity thermogenesis (NEAT)

EAT is planned, structured, and repetitive physical activity with the objective of improving health (participating in a sport like soccer or strength training at the gym, for example).
NEAT is the energy expenditure for unstructured and unplanned activities. This includes daily-living activities like cleaning the house, yard work, shopping, and occupational activities. NEAT also includes the energy required to maintain posture and spontaneous movements such as fidgeting and pacing.2
NEAT can vary by up to 2,000 calories a day for two people of similar size, according to Dr. James Levine, the Mayo Clinic researcher who first coined the term. NEAT may be an important component of obesity prevention and is currently an area of research.
Factors Affecting Energy Intake
Given the importance of energy’s role in sustaining life, it’s not surprising that energy balance is tightly regulated by complex physiological processes. A region in the brain called the hypothalamus is the main control center for hunger and satiety. There is a constant dialogue between our brains and gastrointestinal tracts through hormonal and neural signals, which determine if we feel hungry or full. The hypothalamus can sense nutrient levels in the blood, and when nutrient levels are low, the hunger center is stimulated. Conversely, when nutrient levels are high, the satiety center is stimulated.
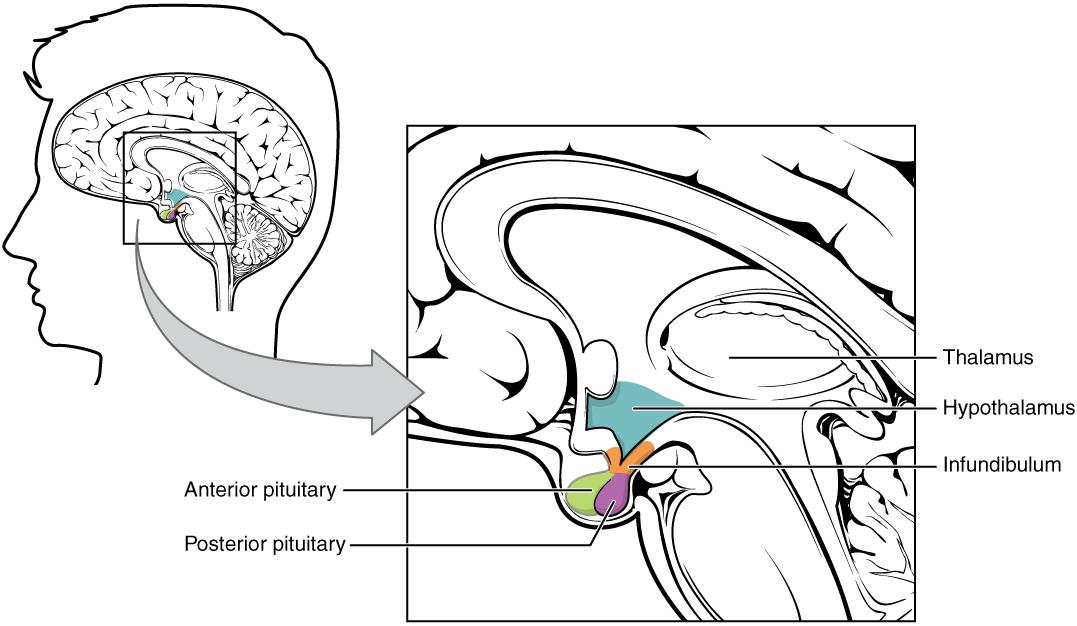
Figure 7.6. The hypothalamus, shown in blue, is about the size of an almond and serves as the hunger center of the brain, receiving signals from the gastrointestinal tract, adipose tissue, and blood and signaling hunger and satiety.
Hunger is the physiological need to eat. When the stomach is empty, it contracts and starts to grumble and growl. The stomach’s mechanical movements relay neural signals to the hypothalamus. (Of course, the stomach also contracts when it’s full and hard at work digesting food, but we can’t hear these movements as well because the stomach’s contents muffle the noise.) The stomach is also the main organ that produces and secretes the “hunger hormone,” ghrelin, the only gut hormone found to increase hunger. Ghrelin levels are high before a meal and fall quickly once nutrients are absorbed.3
Appetite is the psychological desire to eat. Satiety is the sensation of feeling full. After you eat a meal, the stomach stretches and sends a neural signal to the brain stimulating the sensation of satiety and relaying the message to stop eating. There are many hormones that are associated with satiety, and various organs secrete these hormones, including the gastrointestinal tract, pancreas, and adipose tissue. Cholecystokinin (CCK) is an example of one of these satiety hormones and is secreted in response to nutrients in the gut, especially fat and protein. In addition to inhibiting food intake, CCK stimulates pancreatic secretions, gall bladder contractions, and intestinal motility—all of which aide in the digestion of nutrients.3
Adipose tissue also plays a role in regulating food intake. Adipose is the primary organ that produces the hormone leptin, and as fat stores increase, more leptin is produced. Higher levels of leptin communicate to the satiety center in the hypothalamus that the body is in positive energy balance. Leptin acts on the brain to suppress hunger and increase energy expenditure. The discovery of leptin’s functions sparked excitement in the research world and the weight loss industry, as it was hypothesized that leptin might be used as a weight loss drug to decrease food intake. In several clinical trials, it was found that people who are overweight or obese are actually resistant to the hormone, meaning their brain does not respond as well to it. Therefore, when you administer leptin to an overweight or obese person, there is generally no sustained effect on food intake.4
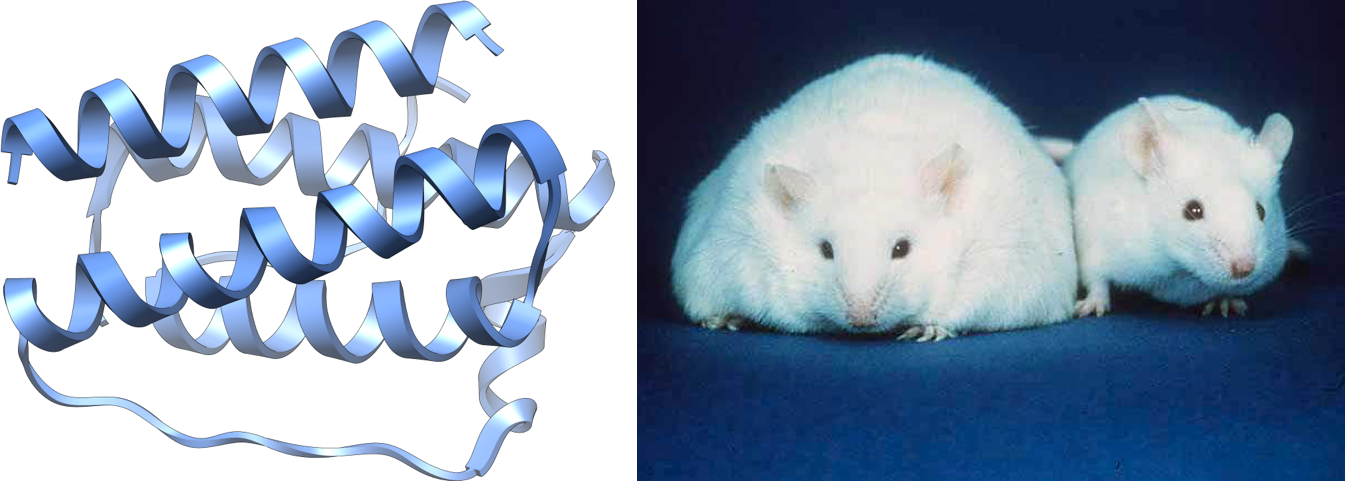
Figure 7.7. The structure of the hormone leptin (left), which is primarily produced by adipose tissue. The obese mouse in the photo has a gene mutation that makes it unable to produce leptin, resulting in constant hunger, lethargy, and severe obesity. For comparison, a mouse with normal leptin production is also shown. Such gene mutations are rare, but they serve as a dramatic illustration of the importance of the hormone in signaling energy balance.
The Complexity of Energy Balance
Energy balance seems like it should be a simple math problem, and in fact, it is based on a fundamental truth in physics—the first law of thermodynamics. This law states that energy can’t be created or destroyed; it can only change form. That is, calories that are consumed must go somewhere, and if they aren’t metabolized (which converts caloric energy to heat and work energy), they’ll have to be stored, usually in the form of adipose tissue. What makes energy balance challenging is the reality that both energy intake and energy expenditure are dynamic variables that are constantly changing, in response to each other and overall energy balance.5,6
Let’s first look at the energy intake side. As we’ve already discussed, how much food we eat each day is not just a matter of willpower or self-control. It’s the result of powerful physiological and psychological forces that tell us if we need to eat, or if we’ve had enough. Our brains are hard-wired to seek food if we’re in negative energy balance, an instinct required for survival. This means that if you start to exercise more—increasing your energy expenditure—you will also feel hungrier, because your body needs more fuel to support the increase in physical activity. If you eat fewer calories, perhaps in an effort to lose weight, your stomach will produce more ghrelin, and your adipose tissue will produce less leptin. These and other shifting hormone levels work together to increase hunger and make you focus on obtaining more calories. People who try to gain weight run into the opposite problem. Their leptin levels increase, suppressing hunger. It’s also uncomfortable to eat beyond satiety, and food doesn’t taste as good once you’re full.
Even measuring how much energy is consumed is not as simple as you might think. We can measure the caloric content of food from a chemical standpoint, but we can only estimate how much energy a person will absorb from that food. This will depend on how well the food is digested and how well the macronutrients are absorbed—factors which vary depending on the food itself, the digestion efficiency of the person eating it, and even the microbes living in their gut. Two people may eat the exact same meal, yet not absorb the same number of calories.
Energy expenditure is also dynamic and changes under different conditions, including increased or decreased caloric intake. Decreased caloric intake and negative energy balance cause a drop in BMR to conserve energy. Muscles also become more efficient, requiring less energy to work, and without realizing it, people in negative energy balance often decrease their NEAT activity level. These adaptations help to conserve body weight and make it more difficult to stay in negative energy balance. People may still be able to lose weight despite their bodies working to prevent it, but maintaining a new, lower weight requires constant vigilance, and weight regain is common.
Research has also shown that people respond differently to positive energy balance. When a group of people are overfed, the amount of weight gained amongst study participants varies widely. In a study of identical twins who were given an extra 1,000 calories per day for 100 days, weight gain varied between 10 and 30 pounds among participants. Weight gain between twins was more similar (though not exactly the same), which may be attributed to genetic factors.7 People gain and lose weight differently; we don’t necessarily follow formulas.
When people say that the answer to weight gain is to eat less and move more, they may be partially correct. But this is also an oversimplified answer, because of all the complexities underlying energy intake and energy expenditure.
Self-check:
References:
- “Balancing Energy Input with Energy Output”, section 11.2 from the book An Introduction to Nutrition (v. 1.0), CC BY-NC-SA 3.0
- 1Webb, D. (2014, November). Farewell to the 3,500-Calorie Rule. Today’s Dietitian, 26(11), 36. https://www.todaysdietitian.com/newarchives/111114p36.shtml
- 2Chun, N., Park, M., Kim, J., Park, H., Hwang, H., Lee, C., Han, J., So, J., Park, J., & Lim, K. (2018). Non-exercise activity thermogenesis (NEAT): a component of total daily expenditure. J Exerc Nutrition Biochem, 22(2), 23–30. doi: 10.20463/jenb.2018.0013
- 3Austin J., & Marks, D. (2008). Hormonal Regulators of Appetite. Int J Pediatr Endocrinol. 2009. doi: 10.1155/2009/141753
- 4Dardeno, T. A. et al. (2010). Leptin in Human Physiology and Therapeutics. Front Neuroendocrinol, 31 (3), 377–93. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2916735/?tool=pubmed
- 5Hall, K. D., & Guo, J. (2017). Obesity Energetics: Body Weight Regulation and the Effects of Diet Composition. Gastroenterology, 152(7), 1718-1727.e3. https://doi.org/10.1053/j.gastro.2017.01.052
- 6Hall, K. D., Heymsfield, S. B., Kemnitz, J. W., Klein, S., Schoeller, D. A., & Speakman, J. R. (2012). Energy balance and its components: Implications for body weight regulation123. The American Journal of Clinical Nutrition, 95(4), 989–994. https://doi.org/10.3945/ajcn.112.036350
- 7Bouchard, C., Tremblan, A.,…Fournier, G. (1990). The response to long-term overfeeding in identical twins. N. Engl. J. Med. 322, 1477-1482.
Images:
- “Energy balance” by Tamberly Powell is licensed under CC BY-NC-SA 2.0 with images used from “Yoga” by Matt Mad is licensed under CC BY-NC-ND 2.0, “Salmon (sustainable fishing), whole grain wild rice, sesame-spinach, avocado, edamame, home-made teriyaki sauce” by Marco Verch is licensed under CC BY 2.0, “Bitten Apple” by DLG Images is licensed under CC BY 2.0, “Exercise” by Andy Cross is licensed under CC BY-NC 2.0, “The Habit: Bacon Cheeseburger” by Person-with-No Name is licensed under CC BY 2.0, and “Watching Gabiera” by Carlos Ebert is licensed under CC BY 2.0
- Fig 7.3. “Components of total energy expenditure” from “Balancing Energy Input with Energy Output,” section 11.2 from the book An Introduction to Nutrition (v. 1.0), CC BY-NC-SA 3.0
- Fig 7.4. “Components of energy expenditure and the percentage they contribute” by Tamberly Powell is licensed under CC BY-NC-SA 2.0
- Fig 7.5. “Energy Expenditure of Organs” by Tamberly Powell is licensed under CC BY-NC-SA 2.0
- Table 7.1. Factors that Impact BMR by Tamberly Powell is licensed under CC BY-NC-SA 2.0
- “Raking Alternative” by Jack Zalium is licensed under CC BY-ND 2.0
- Fig 7.6.“The Hypothalamus-Pituitary Complex” by OpenStax College is licensed under CC BY-SA 3.0
- Fig 7.7. “Leptin” by Vossman is licensed under CC BY-SA 3.0; “Fatmouse” by Human Genome wall for SC99 is in the Public Domain
By this point in the unit, you should understand the types of studies used in nutrition research and the quality of evidence each can provide. As you sift through studies, there are a few limitations of nutrition research that are always worth keeping in mind:
- Challenges in nutrition research: There are some inherent challenges to researching what people eat and how it affects their health. This fact limits the quality of evidence and stirs controversy in nutrition research.
- Influence of food industry funding: Because government funding for nutrition research is limited, much of it is funded by the food industry. Industry’s primary goal is to sell more of their products, so they have a conflict of interest that can result in bias in the way they design studies and interpret the results.
Being alert to these two things means always examining nutrition research with a healthy sense of skepticism. Let’s take a closer look at these two issues in nutrition science.

Challenges in Nutrition Research
How does the food we eat affect our health? This question is exceedingly difficult to answer with certainty. We all need to eat every day, but we can choose from a huge array of possible foods in different combinations. And it’s probably not what we eat on any given day that matters, but what we eat over months and years and decades—our long-term eating patterns—that matter to our long-term health.
Imagine that you’re a nutrition researcher, and you’ve made the observation that over the last 50 years in the U.S., people have been consuming more and more processed foods (foods made with refined ingredients and industrial processes, usually with the addition of sugar, fat, and/or salt). You hypothesize that processed foods are contributing to obesity, which has also increased over the last 50 years. You might first test your hypothesis in animal studies by feeding mice and rats a buffet of potato chips, soda, and Twinkies, and measuring changes in their body weight. You might find that the animals do, in fact, gain weight on this diet. However, you know that what is true in rodents isn’t always true in humans, and you’ll need to study humans in order to understand the role of processed foods in the obesity epidemic.
Your next step might be to conduct an observational study, the most common type of study design in human nutrition research. For example, you might do a cross-sectional study where you compare groups of people who eat a lot of processed foods with those who eat very little. Or you might conduct a prospective cohort study in which you ask people how much processed foods they eat and then follow them over time, looking for correlations between processed food consumption and their body composition.
These types of studies have been conducted, and they’ve found correlations between consumption of processed foods and obesity. For example, a cross-sectional study published in 2018 compared the consumption of processed foods and the prevalence of obesity in 19 European countries and found that countries where people eat more processed foods also have a greater prevalence of obesity.1 A prospective cohort study published in 2016 followed nearly 8,500 university graduates in Spain and found that those who ate more processed foods were more likely to be overweight or obese 9 years later.2
From these results, can we conclude that eating more processed food causes weight gain? Nope. It’s a tempting conclusion, but this brings us to the first major problem with nutrition research: Observational studies can only show that two variables (eating processed foods and obesity, in this case) are correlated, not that one causes the other. This distinction is especially important in nutrition because diet is intertwined with many other lifestyle and socioeconomic factors that also affect health outcomes. For example, people who eat more processed food might also eat fewer fruits and vegetables, exercise or sleep less, have more stress, or have less access to preventative healthcare. These are just a few of the confounding factors that could explain the observed correlation between processed food consumption and weight gain. Weight gain might have nothing to do with processed food and instead be driven by one or all of these factors, or others that we haven’t considered.
The second major problem with observational nutrition research is that it’s difficult to accurately quantify what and how much people eat, especially over long periods of time. Epidemiological studies usually rely on questionnaires that ask people to remember how much food they ate, but people are notoriously bad at remembering this type of information, and sometimes we fudge the truth. For example, you might remember that you had a cup of coffee but forget that you added cream, completely forget about a mid-morning muffin snack, or guess that you ate 2 cups of veggies when it was closer to 1.5 cups. And many diet questionnaires, called food frequency questionnaires, ask people to recollect and mentally average their food and beverage intake for the last 12 months, not just yesterday. The image below shows part of a page from a 24-page National Health and Nutrition Examination Survey (NHANES) food questionnaire, a national survey often used for research on country-wide dietary patterns. As you can see, these questions are detailed, and there’s plenty of room for small errors to accumulate.
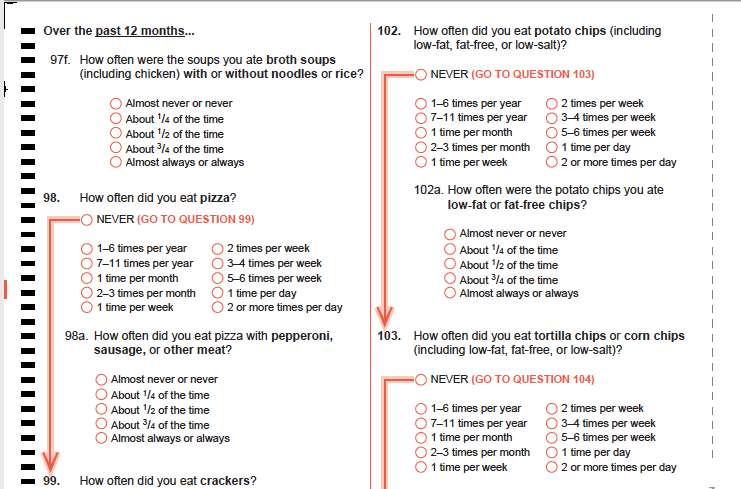
Figure 2.5. A sample page from the NHANES Food Questionnaire.
A third challenge in nutrition research is that diet is just so complex. Stanford physician and researcher John Ioannidis, a frequent critic of observational nutrition research, described the complexity of diet in a 2018 editorial published in JAMA: “Individuals consume thousands of chemicals in millions of possible daily combinations. For instance, there are more than 250,000 different foods and even more potentially edible items, with 300,000 edible plants alone.” He also points out that how an individual responds to a particular dietary pattern can be influenced by genetics, age, and the way they metabolize nutrients. “Disentangling the potential influence on health outcomes of a single dietary component from these other variable is challenging, if not impossible,” Ioannidis wrote.3

Returning to the question of processed foods, all three of these challenges impact how we interpret observational studies that show a correlation between processed food consumption and weight gain. It doesn’t mean that these studies are useless, but we want to be aware of their limitations and consider other ways to test the hypothesis. One way to overcome these challenges is to conduct a randomized controlled trial (RCT), the study design that gives us the highest quality evidence. RCTs are time and funding-intensive experiments, so they’re usually only conducted after consistent evidence from observational and laboratory studies has accumulated.
It turns out that there has been a randomized controlled trial of processed foods and weight gain. It was funded by the National Institutes of Health and published in 2019 in the journal Cell Metabolism.4 In this study, 20 participants lived in the NIH’s Clinical Center for one month, where they consumed only processed foods for two weeks and only unprocessed foods for another two weeks, and they could eat as much or as little as they liked during each of these periods. The diets were carefully designed by dietitians so that they were matched in calories, sugar, fat, fiber, and macronutrients, and the exact amounts consumed by the participants were measured every day (solving the problem of measuring diet complexity and accurately describing what and how much people eat every day).
The study found that people ate about 500 kilocalories more and gained about a pound per week when they were eating processed foods. This study design could show causation, not just correlation, because the other nutritional factors like calories, sugar, fat, fiber, and macronutrients were held constant, and the diets were tested in the same people, so other factors such as genetics, sleep, stress, and exercise were constant between the two types of diets. (This was an example of a crossover randomized controlled trial, in which each subject serves as their own control, and they completed the processed and unprocessed phases of the trial in random order.)

Figure 2.6. At left, researchers Kevin Hall and Stephanie Chung talk with one of the processed foods trial participants at the NIH Clinical Center, an inpatient facility where participants lived for the duration of the study. At right, an NIH worker prepares meals for participants in the center’s kitchen. All meals were provided for study participants to carefully control their diet during the trial.
This study suggested something very important—that food processing causes people to eat more food and gain weight. However, even the best study design has limitations. For one thing, this study was small (just 20 participants), and it only lasted for two weeks, so we don’t know if the findings apply to the general population over a lifetime of complex, ever-changing diets. The next steps will be to try to repeat the study in another group of people to see if the finding holds and to design studies to figure out why processed foods cause increased caloric intake.
As you evaluate nutrition research, especially observational studies, keep in mind the inherent challenges of nutrition research and look for randomized controlled trials that can help solve those challenges. Even for randomized controlled trials, consider their limitations, and know that one study is never enough to fully answer a question in the complex field of nutrition.
Industry Influence: Follow the Money
Understanding how diet influences health is a pressing need. By some estimates, a suboptimal diet is the single greatest changeable risk factor contributing to death and disability worldwide, and in the United States, the cost of diet-related chronic diseases are estimated to be as high as $1 trillion each year.5 Yet, for all its importance, nutrition science has long suffered from a lack of government investment, with only about 5 percent of the National Institutes of Health (NIH) budget, or $1.8 billion, directed towards research on how the foods we eat affect our health, according to a 2019 investigation by Politico. “In 2018, NIH funding for cancer, which affects just under 9 percent of the population, was $6.3 billion. Funding for obesity, which affects about 30 percent of the country, was about $1 billion,” the article noted.6
With so little government funding for nutrition science, who is funding the rest of the studies that feed the constant news cycle? Many are funded by food companies and industry groups, either to conduct studies in their own research divisions or in the form of grants given to university scientists. That’s problematic, because food companies and industry groups have an inherent bias or conflict of interest. Their primary goal is to promote their products and to sell more of them—not to advance knowledge of food and health—and this affects how they frame research questions, design and interpret studies, and report their results.
Marion Nestle, a retired nutrition professor at New York University, has written extensively about this problem. For a year in 2015-2016, she informally tracked industry-funded studies and found that 90 percent of the time, their conclusions benefitted the industry that funded them. In another example, a 2013 meta-analysis found that among studies that looked at whether soda consumption contributed to obesity, those funded by the soda industry were five times more likely to conclude that it doesn’t contribute to obesity compared to those not funded by the industry.7 (Consider the processed foods RCT we just discussed. It was funded by the National Institutes of Health, which doesn’t have a stake in the results. Would you trust the results of a study of processed foods if it was funded by Nabisco? Or for that matter, the Broccoli Growers of America? Probably not.)
There’s likely a long history of biased nutrition research influencing dietary advice. For example, in the 1960s, the sugar industry paid well-respected academic scientists to publish research concluding that it was fat—not sugar—that was detrimental to heart health.8 (Both too much fat and too much sugar can negatively affect heart health, but it benefited the sugar industry to focus the blame on fat.) As recently as 2015, Coca-Cola was funding research meant to promote lack of physical activity as the main cause of obesity, shifting blame away from dietary factors, such as drinking soda.9 When food companies drive the narrative coming out of nutrition research, this can potentially impact public policy.
Media attention has made researchers and policy makers much more aware of the problems with industry funding and conflicts of interest in nutrition research, and they’re working to solve them. But regardless, if you see reports of a study that shows that blueberries can block bladder infections, pistachios can prevent pancreatitis, or cinnamon can cure cancer… well, you should be skeptical, and always check the funding source. Studies on a single type of food are almost always industry-funded.
How to find clarity in a complex field
Let’s review some of the key issues:
- Nutrition research is really difficult to do well. We want to know how nutrition relates to health over the long term, but it’s hard to quantify how people eat over a lifetime and track them for long enough to see an impact.
- We often rely on observational studies, which can only show that two variables are correlated, not that one causes the other.
- Randomized controlled trials are rare, and they’re often small, short-term studies that may or may not tell us what happens in the real world.
- Diet is exceptionally complex, with countless combinations of different nutrients and foods.
- One study is never enough to fully answer a question in the complex field of nutrition.
- Nutrition research is often funded by the food industry, which can be biased towards results that benefit business, not human health.
All of this can be discouraging, but you should also know that researchers are working hard to improve the quality of nutrition research and to interpret it honestly for the rest of us. As a consumer of nutrition information, use a skeptical eye when you read news of the latest nutrition research. Look for areas of consensus, where committees of experts have put their heads together to come up with the best advice they can based on the evidence we have, such as in the Dietary Guidelines for Americans. You’ll find that while experts in this field are often debating the latest controversy, they also agree on a lot. As we continue on in this unit, we’ll talk more about how to find accurate sources of information and who you can trust for evidence-based advice in the field of nutrition.
Self-Check:
References
- 1Monteiro, C. A., Moubarac, J.-C., Levy, R. B., Canella, D. S., Louzada, M. L. da C., & Cannon, G. (2018). Household availability of ultra-processed foods and obesity in nineteen European countries. Public Health Nutrition, 21(1), 18–26. https://doi.org/10.1017/S1368980017001379
- 2Mendonça, R. de D., Pimenta, A. M., Gea, A., de la Fuente-Arrillaga, C., Martinez-Gonzalez, M. A., Lopes, A. C. S., & Bes-Rastrollo, M. (2016). Ultraprocessed food consumption and risk of overweight and obesity: The University of Navarra Follow-Up (SUN) cohort study. The American Journal of Clinical Nutrition, 104(5), 1433–1440. https://doi.org/10.3945/ajcn.116.135004
- 3Ioannidis, J. P. A. (2018). The Challenge of Reforming Nutritional Epidemiologic Research. JAMA, 320(10), 969–970. https://doi.org/10.1001/jama.2018.11025
- 4Hall, K. D., Ayuketah, A., Brychta, R., Cai, H., Cassimatis, T., Chen, K. Y., Chung, S. T., Costa, E., Courville, A., Darcey, V., Fletcher, L. A., Forde, C. G., Gharib, A. M., Guo, J., Howard, R., Joseph, P. V., McGehee, S., Ouwerkerk, R., Raisinger, K., … Zhou, M. (2019). Ultra-Processed Diets Cause Excess Calorie Intake and Weight Gain: An Inpatient Randomized Controlled Trial of Ad Libitum Food Intake. Cell Metabolism, 30(1), 67-77.e3. https://doi.org/10.1016/j.cmet.2019.05.008
- 5Mozaffarian, D. (2017). Conflict of Interest and the Role of the Food Industry in Nutrition Research. JAMA, 317(17), 1755–1756. https://doi.org/10.1001/jama.2017.3456
- 6Boudreau, C., & Evich, H. B. (n.d.). How Washington keeps America sick and fat. POLITICO. Retrieved January 27, 2020, from https://www.politico.com/news/agenda/2019/11/04/why-we-dont-know-what-to-eat-060299
- 7Bes-Rastrollo, M., Schulze, M. B., Ruiz-Canela, M., & Martinez-Gonzalez, M. A. (2013). Financial Conflicts of Interest and Reporting Bias Regarding the Association between Sugar-Sweetened Beverages and Weight Gain: A Systematic Review of Systematic Reviews. PLOS Medicine, 10(12), e1001578. https://doi.org/10.1371/journal.pmed.1001578
- 8Kearns, C. E., Schmidt, L. A., & Glantz, S. A. (2016). Sugar Industry and Coronary Heart Disease Research: A Historical Analysis of Internal Industry Documents. JAMA Internal Medicine, 176(11), 1680–1685. https://doi.org/10.1001/jamainternmed.2016.5394
- 9O’Connor, A. (2015, August 9). Coca-Cola Funds Scientists Who Shift Blame for Obesity Away From Bad Diets. The New York Times. https://well.blogs.nytimes.com/2015/08/09/coca-cola-funds-scientists-who-shift-blame-for-obesity-away-from-bad-diets/
Image Credits
- “Magnifying glass” photo by Emiliano Vittoriosi on Unsplash (license information)
- Figure 2.5.”NHANES food questionnaire” by CDC is in the public domain
- “Table of food photo” by Spencer Davis on Unsplash (license information)
- Figure 2.6. “NIH study center photos” by Jennifer Rymaruk, NIDDK are in the Public Domain

{kind=link}
{kind=link}
{kind=link}