Universal Health Coverage: The Benefits of Implementation in the United States
Colette Feghali-Behboud
Personal Statement
I am a current public health student at Lake Washington Institute of Technology. My purpose for developing this research paper is to bring awareness to the advantages and challenges of implementing a universal health coverage system in the United States. Despite the challenges, change is possible and recommended to improve health equity and increase general productivity among residents and communities. As a future public health professional, I aim to advocate for health reform in the state of Washington so that health care is accessible and affordable to all populations. Health care is a basic human right, not a privilege.
Abstract
This paper aims to address how universal health coverage (UHC) could impact the quality of life for middle- to low-income households in the United States. The approaches to addressing this issue include gathering empirical data from credible sources and providing successful examples from other countries that utilize this type of system. Information on the advantages and challenges of UHC implementation in the U.S. have been collected and will be discussed. A few examples of advantages include health equity, improved quality of life for all, and decreased financial burdens for vulnerable populations. With the implementation of a UHC system in the U.S., it could foster a more productive society.
As one of the wealthiest nations in the world, the United States and its government should be able to provide Americans with universal health coverage (UHC). Many countries have successfully implemented some form of UHC and have statistically spent less money on health care services compared to the U.S. (McGough et al., 2023, para. 2). Universal health care has many benefits that could drastically transform and save lives. Based on evidence from comparably wealthy countries, once established, UHC in the U.S. would provide improved quality of life and health equity, preventive health care, affordable and cost-effective medical coverage, protection against future outbreaks and preventable deaths, and a better health care system. Quality health care should be easily accessible by all residents of the U.S.
Quality of Life and Health Equity Improvements
A common statement that many people believe, and others should acknowledge, is this: health care is a basic human right, not a privilege. According to the World Health Organization (WHO), universal health care is “ensuring that all people have access to needed health services (including prevention, promotion, treatment, rehabilitation and palliation) of sufficient quality to be effective while also ensuring that the use of these services does not expose the user [to] financial hardship” (Zieff et al., 2020, para. 2). Developing a UHC system in the U.S. would improve quality of life by eliminating medical costs incurred by uninsured and vulnerable populations. Additionally, a UHC system provides flexibility for people to pursue better employment as they are not tied to employer-provided insurance. A substantial portion of the U.S. population receives medical insurance through their employers and can thus face substantial hardships when losing employment. This is especially true among vulnerable populations that tend to have lower employment percentages. By providing UHC, health equity may be improved by narrowing the income-related disparities inherent in the U.S. (Schneider et al. 2021, para. 23). The quality of life for Americans can be improved by preventive care, which can diagnose and treat diseases before they become life-threatening (Galvani et al., 2020, para 19).
Advantages of Sustaining Preventive Health Care
One of the most important impacts of UHC is preventive care through access to healthcare services among middle- and low-income populations who cannot currently pay for medical costs. Patients who are at risk for developing chronic diseases and illnesses can address them at regular doctor visits and screenings. According to Zieff et al. (2020), “Accessible, affordable healthcare may enable earlier intervention to prevent—or limit risk associated with—non-communicable chronic diseases, improve the overall public health of the U.S., and decrease the economic strain associated with an unhealthy low-SES [socioeconomic status]” (para. 8). With the current costs of private insurance and unreliable employer-based health care, vulnerable populations are often underinsured or uninsured. This results in certain populations becoming unhealthy and less productive. Some examples of benefits that would be managed under UHC include behavioral and mental-health disorders, substance-use disorders, communicable diseases, and non-communicable diseases such as heart disease, diabetes, and cancer (American Academy, n.d., Benefits section). Routine preventive care can foster an environment for patients to receive ongoing care and screenings as they age, including mammograms and prostate exams. With preventive care, patients with non-communicable diseases can receive laboratory and diagnostic testing to prevent emergency room visits. Supporting this approach, Zieff et al. (2020) report that “the uninsured diabetic population is responsible for 55% more emergency room visits each year than their insured diabetic counterparts” (para. 8). If the U.S. government adopted a UHC system, these conditions could be prevented or treated without any financial burdens associated with medical costs.
Affordable and Cost-Effective Medical Coverage
Americans who are against the implementation of UHC in the U.S. claim that the financial costs do not outweigh the benefits. On the contrary, Galvani et al. (2020) state, “we predict that a single-payer healthcare system would require $3.034 trillion annually, $458 billion less than current national healthcare expenditure” (para. 12). This translates into a savings of ~$1,400 per person annually. Additionally, the existing U.S. healthcare system already spends a disproportionate amount of gross domestic product (GDP) on medical care compared to economically comparable nations. A study that analyzed the U.S. healthcare costs per GDP found that “health spending per person in the U.S. was $12,914 in 2021, which was over $5,000 more than any other high-income nation” (McGough et al., 2023, para. 4)(see Figure 1). The U.S. is spending approximately 17% of its GDP on health care compared to 8 to 12% among 10 other wealthy nations, yet the care in the U.S. is substantially worse (Schneider et al., 2021, Exhibit 4). The one aspect of the current U.S. healthcare system that is working well is the “rates of mammography screening and influenza vaccination as well as the percentage of adults who [spoke] with their provider about nutrition, smoking, and alcohol use” (Schneider et al., 2021, para. 19). When advocating for the implementation of UHC in the U.S., it will be important to preserve this aspect that is currently working well.
Further objections to the UHC system are often made by shareholders of insurance companies whose primary focus is to drive up the price value of shares. Due to the insurance companies’ fiduciary responsibility to their shareholders combined with the private insurance model that has transiently enrolled patients, long-term care is not a priority. Instead, by limiting primary care, they reduce short-term costs (Galvani et al., 2020, para. 19). Under the UHC model, “a single-payer system would be financially responsible for healthcare throughout the lifespan of all Americans, [and thus] it becomes efficient to incur a small cost in the present with the purpose of avoiding more serious and costly health conditions in the future” (Galvani et al., 2020, para. 19). Associated costs with administrative, medical-service, and other health-care fees would decrease, and can balance the initial financial burden of establishing such a system. Along these lines, vulnerable groups would be able to access primary care and potentially save their lives.
Protection Against Future Outbreaks and Preventable Deaths
During the COVID-19 pandemic, many Americans had insufficient access to medical coverage, which led to high mortality rates. Galvani et al. (2022) calculated that about 338,954 preventable deaths associated with the COVID-19 pandemic could have been averted with a UHC system (para. 11). For instance, if the uninsured populations had medical coverage and had been able to maintain health issues, it would have lowered their risk of comorbidities and death during the pandemic. According to the policy statement from the APHA, the existing employer-sponsored health insurance is subject to downturns in the economy and was predicted to cause 10 million Americans to lose their insurance from being laid off during the Covid-19 pandemic (American Public Health Association [APHA], 2020, para. 7). As a result, many Americans and family members enrolled into Medicaid/Children’s Health Insurance Program (CHIP), further straining state and federal budgets (APHA, 2020, para. 5)(see Figure 2).
When Americans lose their access to health care, they can become vulnerable to mortality due to outbreaks as their diseases and illnesses go untreated. It is unsurprising that the tragic result of the Covid-19 pandemic in the U.S. was, in the estimation of Galvani et al (2020), that “the number of lives that could have been saved in 2020 by universal healthcare from both non-COVID conditions and COVID-19 would be 211,897” (para. 12). The American Public Health Association (APHA) (2020) describes the pandemic as “a watershed moment where we can reconstruct a fractured health insurance system into a system of universal health care” (Problem Statement section, para. 15). In the words of Wesley Mantooth, a professor and department chair at Lake Washington Institute of Technology, “in terms of communicable diseases, it seems like [the case for implementing UHC] is a good argument to persuade people that all of society would be safer if currently vulnerable members had better care” (Mantooth, personal communication, March 8th, 2023). To address this issue of inequity in the U.S. healthcare system, many people advocate for a transition to UHC. For example, Senator Bernie Sanders supports the Medicare for All Act (MAA), which would lower maternal deaths, increase the rate of survival for newborns, and increase the longevity of all people in the U.S. who are currently dying without comprehensive medical care (Galvani et al., 2020, Introduction section). Unfortunately, the reform in the U.S. healthcare system is slow to evolve and is often mired in political misinformation.
Successful Coverage Among Other Comparably Wealthy Countries
Despite being one of the highest income countries, the U.S. ranks among the lowest in healthcare approaches compared to countries with UHC. A 2021 study compared healthcare systems in 11 wealthy nations: Australia, Canada, France, Germany, Netherlands, New Zealand, Norway, Sweden, Switzerland, and the U.S. According to Schneider et al. (2021), the key differences can be summarized below:
Four features distinguish top-performing countries from the United States: 1) they provide for universal coverage and remove cost barriers; 2) they invest in primary care systems to ensure that high-value services are equitably available in all communities to all people; 3) they reduce administrative burdens that divert time, efforts, and spending from health improvement efforts; and 4) they invest in social services, especially for children and working-age adults. (para. 5)
For the U.S. to reach equal standards of care, these four features must be addressed:
- Providing affordable, universal coverage helps with three subcategories of care. First, patients would be less likely to report that insurance companies denied their claims. Secondly, patients would have fewer burdens in paying for their care. Lastly, there would be better access to same-day care as well as after-hours care. Currently, the U.S. ranks last when compared to 10 other wealthy nations in providing affordable coverage (Schneider et al., 2021, para. 14).
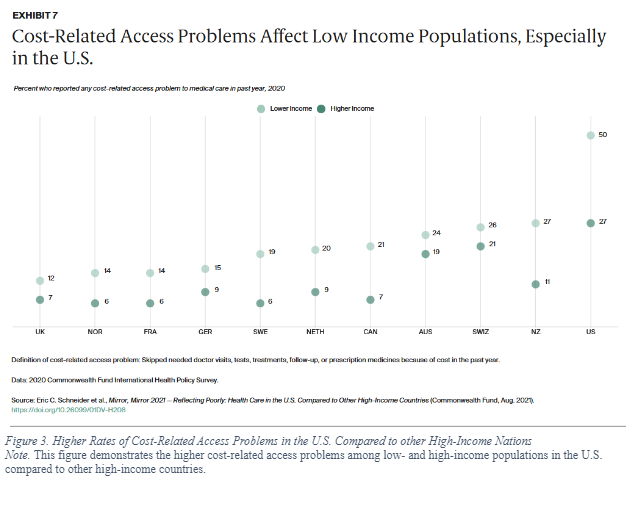
- The next feature is equitably available primary care, which is currently unbalanced in the U.S., with high-income patients reporting easier access to primary care, while low-income communities struggle to meet their needs. When comparing the income gap to access of care of these same 10 wealthy nations, it becomes clear that not only would low-income communities benefit from UHC, but also wealthier ones, as 27% of high-income U.S residents still report access problems (Schneider et al., 2021, Exhibit 7) (see Figure 3). To clarify, this means that even wealthy communities would gain ground with the transition to UHC.
- In the pursuit of improving administrative efficiencies, the U.S. stands to benefit from UHC implementation, as the U.S. ranks last in this category as well. Administrative efficiency is a measure of how burdensome documentation and bureaucratic tasks are that impose difficulties for patients and doctors to pursue care. Since insurance in the U.S. is so fragmented, patients can experience roadblocks to medication or treatment because their insurance does not cover it, or because a specialty clinic is out-of-network. By eliminating these inefficiencies with the implementation of UHC, the U.S. can reduce the cost of care and manage primary care efficiently and effectively.
- The final category that these other wealthy countries currently outpace the U.S. in is their investment in social services. These services include “access to nutrition, education, child care, community safety, housing, transportation, and worker benefits” (Schneider et al., 2021, Discussion section). The benefits of these services contribute to one critical aspect of health care: a healthier population that lessens the burden on health services. A metaphor can be used to illustrate this concept, where the “reduce” feature of the “reduce, re-use, and recycle” program moto aims to prevent the use of materials before they enter the production cycle. Similarly, reducing hospital and emergency room visits by promoting healthier and more equitable communities in the first place can save money and resources. In a country where a large part of the GDP is already spent on health care, saving costs by moving to UHC would benefit the whole populace. It is important that all Americans can afford medical care to achieve the best health possible.
Conclusion
Health care in the U.S. is lacking and should reform to universal coverage as successfully shown in other comparable countries. Although universal health coverage has its advantages and disadvantages, the disadvantages of the initial financial costs would eventually balance out over time. Many advantages include access to health care for all, prevention of chronic diseases and illnesses, reduced medical bills, and protection against future national emergencies. Universal coverage provides access to health care for those without means to currently afford the costs. It would improve the health of the general population by providing routine care, preventive care, treatment, and support and resources to maintain their current conditions. Additionally, with the elimination of financial burdens from medical fees, middle- to low-income households would be able to provide their families with basic needs such as food and housing, among other things. Eliminating employer-sponsored health coverage would allow companies to divert their insurance payments to the paychecks of their workers. While workers would need to adjust to higher taxes to cover UHC, they would still save an expected $1,400 annually, per person, which may then be used to further stimulate the economy. This change could bring about better health and better economic growth.
References
American Academy of Family Physicians (n.d.). Health care for all: A framework for moving to a primary care-based health care system in the United States. American Academy of Family Physicians (AAFP). https://www.aafp.org/about/policies/all/health-care-for-all.html
American Public Health Association (2020, October 24). The importance of universal health care in improving our nation’s response to pandemics and health disparities. American Public Health Association (APHA). https://www.apha.org/Policies-and-Advocacy/Public-Health-Policy-Statements/Policy-Database/2021/01/14/The-Importance-of-Universal-Health-Care-in-Improving-Response-to-Pandemics-and-Health-Disparities
Galvani, A. P., Parpia, A. S., Foster, E. M., Singer, B. H., & Fitzpatrick, M. C. (2020). Improving the prognosis of health care in the USA. The Lancet, 395(10223), 524–533. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8572548/
Galvani, A. P., Parpia, A. S., Pandey, A., Sah, P., Colón, K., Friedman, G., Campbell, T., Kahn, J. G., Singer, B. H., & Fitzpatrick, M. C. (2022). Universal healthcare as pandemic preparedness: The lives and costs that could have been saved during the COVID-19 pandemic. Proceedings of the National Academy of Sciences, 119(25). https://doi.org/10.1073/pnas.2200536119
McGough, M., Telesford I., Rakshit, S., Wager, E., Amin, K., & Cox, C. (2023, February 15). How does health spending in the U.S. compare to other countries? Peterson-KFF Health System Tracker. https://www.healthsystemtracker.org/chart-collection/health-spending-u-s-compare-countries/
Schneider, E. C., Shah, A., Doty, M. M., Tikkanen, R., Fields, K., & Williams II, R. D., (2021) Mirror, mirror 2021: Reflecting poorly. Commonwealth Fund. https://doi.org/10.26099/01dv-h208
Zieff, G., Kerr, Z. Y., Moore, J. B., & Stoner, L. (2020). Universal healthcare in the United States of America: A healthy debate. Medicina-Lithuania, 56(11), 580. https://doi.org/10.3390/medicina56110580
Appendix
Note. This figure demonstrates the higher cost-related access problems among low- and high-income populations in the U.S. compared to other high-income countries.
Figure 1. U.S. Health Care Costs per GDP Compared to Other High-Income Nations
Note. This figure shows a comparison of health-care costs per GDP between the U.S. and other high-income nations.
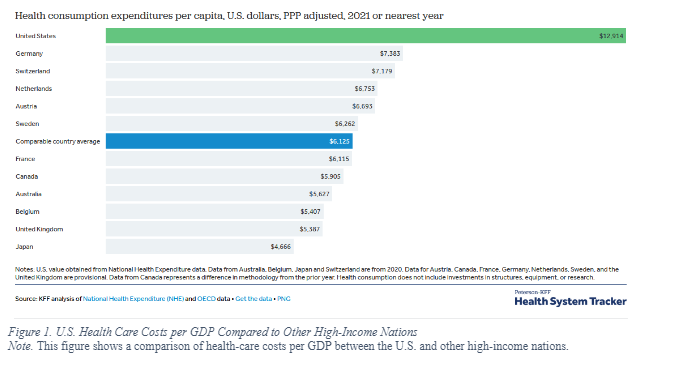
Figure 2. Medicaid/Children’s Health Insurance Program (CHIP) Enrollment (A, B), Excess Death (C), and Years of Life Lost (D) During Covid-19 Pandemic
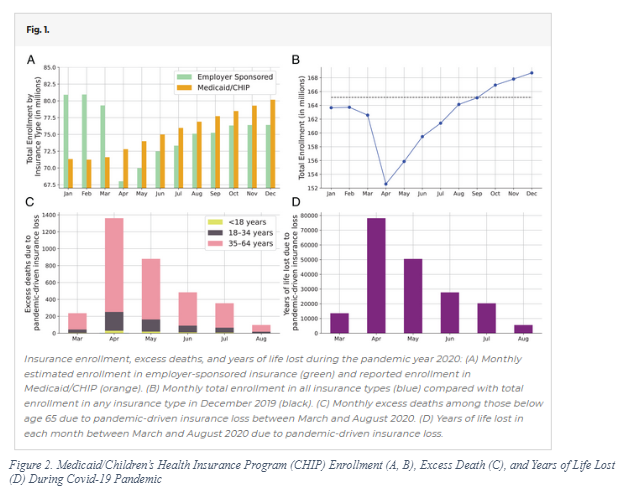
Figure 3. Higher Rates of Cost-Related Access Problems in the U.S. Compared to other High-Income Nations
Note. This figure demonstrates the higher cost-related access problems among low- and high-income populations in the U.S. compared to other high-income countries.
Keywords: universal health care; universal health coverage; health care; health care systems; health care debate; health care costs; health equity; universal health care benefits; universal health care advantages; access to health care
